

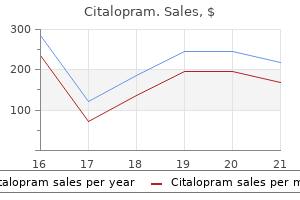
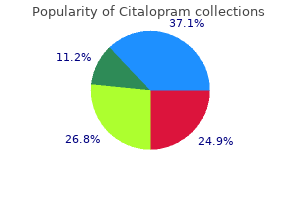
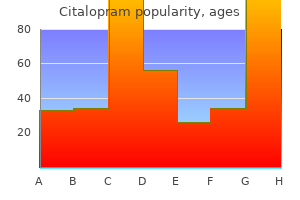
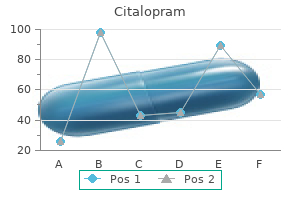
Citalopram
Catherine Cordonnier, M.D.
- Professor of Hematology
- Hematology Oncology
- Universit? Paris 12
- Head
- Clinical Hematology Department
- Henri Mondor University Hospital
- Cr?teil, France
Citalopram dosages: 40 mg, 20 mg
Citalopram packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy citalopram 40mg mastercard
Basophils are a kind of circulating granulocyte that expresses highaffinity Fc receptors and incorporates granules with contents just like treatment urinary tract infection purchase 40mg citalopram visa these of mast cells treatment 02 binh generic citalopram 40mg online. On binding of antigen to IgE on the floor of mast cells or basophils medicine 0829085 purchase 20 mg citalopram with amex, the high-affinity Fc receptors turn into cross-linked and activate intracellular second messengers that result in granule release and new synthesis of mediators. Y Y speedy vascular and clean muscle reactions of instant hypersensitivity, similar to vasodilation, vascular leakage and edema, bronchoconstriction, and intestine hypermotility. Cytokines launched by mast cells and Th2 cells mediate the late-phase reaction, which is an inflammatory reaction involving neutrophil and eosinophil infiltration. Susceptibly to allergic diseases is inherited, and allelic variations of a number of genes have been related to allergic bronchial asthma. Various organs present distinct forms of instant hypersensitivity involving different mediators and target cell varieties. Asthma is a manifestation of immediate hypersensitivity and late-phase reactions in the lung. Allergic rhinitis (hay fever) is the most common allergic illness of the higher respiratory tract. In the skin, instant hypersensitivity is manifested as wheal-andflare and late-phase reactions and should lead to continual eczema. Drug therapy is aimed at inhibiting mast cell mediator production and at blocking or counteracting the consequences of released mediators on track organs. The aim of immunotherapy is to forestall or reduce Th2 cell responses to specific allergens and the manufacturing of IgE. Immediate hypersensitivity reactions provide protection against helminthic infections by promoting IgE- and eosinophil-mediated antibody-dependent cell-mediated cytotoxicity and intestine peristalsis. Mast cells may also play a job in innate immune responses to bacterial infections. Asthma as a continual disease of the innate and adaptive immune methods responding to viruses and allergens. This chapter describes the major types of congenital and purchased immunodeficiencies, with an emphasis on their pathogenesis and the components of the immune system which are concerned in these problems. The principal consequence of immunodeficiency is elevated susceptibility to infection. Deficient humoral immunity often leads to infection by encapsulated, pus-forming bacteria and a few viruses, whereas defects in cell-mediated immunity result in an infection by viruses and different intracellular microbes or the reactivation of latent infections. Combined deficiencies in each humoral and cell-mediated immunity make patients susceptible to an infection by all lessons of microorganisms. Immunodeficient sufferers, particularly those with defects in mobile immunity, typically present with infections by microbes which are commonly encountered but effectively eliminated by wholesome individuals; such infections are said to be opportunistic. Defects in innate immunity can outcome in infections by different categories of microbes, relying on the pathway or cell sort affected. There is rising evidence that adults with recurrent or extreme infections often harbor mutations in genes that regulate immune operate. Defects in one or more elements of the immune system can lead to critical and sometimes fatal problems, which are collectively called immunodeficiency illnesses. This statement suggests that in humans, different mechanisms are often critical for defense against different pathogens, so that defects in anybody mechanism make people susceptible to only some infections. An elevated incidence of most cancers is most often seen in T cell immunodeficiencies as a end result of, as discussed in Chapter 18, T cells play an essential role in surveillance towards malignant tumors. Paradoxically, certain immunodeficiencies are associated with an elevated incidence of autoimmunity. It can be attainable that the persistent infections related to immunodeficiencies cause innate immune activation and tissue damage and promote the activation of autoreactive lymphocytes. Immunodeficiency could result from defects in lymphocyte development or activation or from defects in the effector mechanisms of innate and adaptive immunity. Immunodeficiency diseases are clinically and pathologically heterogeneous, partly because totally different diseases involve totally different components of the immune system. Abnormalities in lymphocyte development may be caused by mutations in genes encoding enzymes, adaptors, transport proteins, and transcription factors. These inherited defects, and the corresponding targeted disruptions in mice, have been instructive in elucidating mechanisms of lymphocyte improvement and performance (see Chapter 8). In this chapter, we first describe primary (congenital) immunodeficiencies, including defects in components of the innate immune system and defects in the humoral and cell-mediated arms of the adaptive immune system. Primary immunodeficiencies generally come to mild due to a clinical history of repeated infections. Some diagnoses are comparatively easily made by measurement of serum immunoglobulin (Ig) ranges, move cytometry of immune cells, or assessment of neutrophil perform in vitro. However, more detailed investigations usually prove essential to obtain an accurate analysis. This assay is used to diagnose severe mixed immunodeficiency, discussed later, instantly after birth and permits for well timed correction of the defect by hematopoietic stem cell transplantation. Many of the identified mutations are listed within the tables, and chosen ones are described in the textual content. Defects in Innate Immunity Innate immunity constitutes the first line of defense in opposition to infectious organisms. Two necessary elements Primary (Congenital) Immunodeficiencies 461 of innate immunity are phagocytes and complement, both of which also take part in the effector section of adaptive immunity. Therefore, congenital issues of phagocytes and the complement system lead to recurrent infections. Phagocyte defects usually lead to infections of the skin and respiratory tract with bacteria or fungi, the latter predominantly involving Aspergillus and Candida species. It is a uncommon disease, estimated to affect roughly 1 in 200,000 individuals within the United States. Approximately two-thirds of instances show an X-linked recessive pattern of inheritance, and the remainder are autosomal recessive. This mutation results in faulty production of superoxide anion, certainly one of a quantity of reactive oxygen species that constitute a significant microbicidal mechanism of phagocytes, particularly neutrophils (see Chapter 4). Defective production of reactive oxygen species results in a failure to kill phagocytosed microbes. The disease was typically fatal up to now, even with aggressive antibiotic remedy, however the prognosis has improved considerably now because of earlier recognition and higher management of infections. After neutrophil superoxide production is restored to approximately 10% of regular ranges, resistance to an infection is greatly improved. Leukocyte Adhesion Deficiencies the leukocyte adhesion deficiencies are a group of autosomal recessive disorders brought on by defects in leukocyte and endothelial adhesion molecules. These illnesses are characterised by a failure of leukocyte, significantly neutrophil, recruitment to sites of infection, resulting in severe periodontitis and different recurrent infections starting early in life, and an inability to make pus. Different forms of leukocyte adhesion deficiencies are caused by mutations in several genes. The absence of sialyl Lewis X leads to defective attachment of leukocytes to endothelium, the absence of leukocyte rolling, and therefore the faulty recruitment of leukocytes to sites of an infection. Patients present with severe infections with viruses mainly of the herpesvirus and papillomavirus households. Ch�diak-Higashi syndrome is a uncommon autosomal recessive dysfunction characterized by recurrent infections by pyogenic micro organism, partial oculocutaneous albinism, and infiltration of varied organs by nonneoplastic lymphocytes.
Citalopram 40mg lowest price
Cytokine therapies medications for rheumatoid arthritis proven 20 mg citalopram, discussed earlier symptoms 6 days after iui cheap citalopram 40 mg without a prescription, represent another methodology of enhancing immune responses in a nonspecific method medicine 100 years ago order citalopram 20mg line. The challenge in use of this remedy to enhance clinical outcome is to minimize the harmful graftversus-host disease that might be mediated by the identical donor T cells (see Chapter 17). The exceptional recent advances in most cancers immunotherapy promise to dramatically change the care of sufferers with these dreaded diseases. Although limitations and problems remain, the enormous effort being invested in this field makes it doubtless that further advances will occur rapidly. Other Approaches for Stimulating Antitumor Immunity Several additional approaches have been used to improve host immunity in opposition to tumors, with variable success. Many cytokines even have the potential to induce nonspecific inflammatory responses, which by themselves may have antitumor activity. Antibodies particular for tumor cell antigens are used for analysis, and the antigens are potential targets for antibody remedy. These antigens include oncofetal antigens, which are expressed normally during fetal life and whose expression is dysregulated in some tumors; altered surface glycoproteins and glycolipids; and molecules which may be usually expressed on the cells from which the tumors arise and are thus differentiation antigens for particular cell types. Tumor-associated macrophages and myeloid-derived suppressor cells, found in most solid tumors, can suppress antitumor immunity. Immunotherapy for tumors is designed to augment active immune responses in opposition to these tumors or to administer tumor-specific immune effectors to patients. Immune responses can also be actively stimulated by vaccination with tumor cells or antigens, and by systemic administration of cytokines that stimulate immune responses. In checkpoint blockade, antibodies against inhibitory receptors on T cells or their ligands are administered to take away the brakes on lymphocyte activation and thus promote antitumor immunity by beforehand inhibited host T cells specific for tumor antigens. The continuum of cancer immunosurveillance: prognostic, predictive, and mechanistic signatures. The position of neoantigens in naturally occurring and therapeutically induced immune responses to cancer. The Role of Neoantigens in Naturally Occurring and Therapeutically Induced Immune Responses to Cancer. In these situations, the usually beneficial immune response is the reason for disease. We will conclude with a quick consideration of the remedy of immunologic illnesses and examples of ailments that illustrate necessary principles. This term arose from the scientific definition of immunity as sensitivity, which relies on the statement that an individual who has been exposed to an antigen displays a detectable reaction, or is sensitive, to subsequent encounters with that antigen. Normally, immune responses eradicate infectious pathogens with out critical injury to host tissues. Autoimmune illnesses are estimated to affect at least 2% to 5% of the population in developed countries, and the incidence of these issues is rising. Autoimmune diseases are often chronic and infrequently debilitating, and an unlimited medical and economic burden. Although these problems have been tough to treat up to now, many new effective therapies have been developed since the 1990s based mostly on scientific rules. Immune responses towards microbial antigens could cause disease if the reactions are extreme or the microbes are unusually persistent. T cell responses against persistent microbes could give rise to severe irritation, generally with the formation of granulomas; this is the cause of tissue damage in tuberculosis and some other persistent infections. If antibodies are produced against microbial antigens, the antibodies may bind to the antigens to 417 418 Chapter 19 � Hypersensitivity Disorders � produce immune complexes, which deposit in tissues and set off irritation. Rarely, antibodies or T cells towards a microbe will cross-react with a bunch tissue. Sometimes the mechanisms that an immune response makes use of to eradicate a pathogenic microbe require killing infected cells, and subsequently such responses inevitably injure host tissues. These individuals produce immunoglobulin E (IgE) antibodies that cause allergic illnesses (see Chapter 20). Some people turn out to be sensitized to environmental antigens and chemicals that contact the skin and develop T cell reactions that result in cytokine-mediated irritation, resulting in contact sensitivity. Idiosyncratic immunologic reactions against therapeutic drugs are additionally a frequent medical problem. Because the stimuli for these irregular immune responses are often unimaginable to eliminate. Therefore, these hypersensitivity diseases are likely to be persistent and progressive and pose major therapeutic challenges in medical medicine. These mechanisms embrace some which are predominantly dependent on antibodies and others predominantly dependent on T cells, though a role for both humoral and cell-mediated immunity is often discovered in plenty of hypersensitivity ailments. We will briefly go over the classification of these illnesses, after which contemplate antibody-mediated and T cell�mediated ailments in higher element. In all of those situations, the mechanisms of tissue damage are the same as those that normally perform to eliminate infectious pathogens. These mechanisms include innate and adaptive immune responses involving phagocytes, antibodies, T lymphocytes, mast cells, and varied different effector cells, and mediators of irritation. Diseases Caused by Antibodies 419 � � � will most likely be discussed in detail individually in Chapter 20. IgG and IgM antibodies particular for cell floor or extracellular matrix antigens may cause tissue harm by activating the complement system, by recruiting inflammatory cells, and by interfering with regular mobile features. IgM and IgG antibodies particular for soluble antigens within the blood type complexes with the antigens, and the immune complexes may deposit in blood vessel partitions in various tissues, inflicting inflammation, thrombosis, and tissue harm. In these problems, tissue damage could also be as a end result of T lymphocytes that induce irritation or instantly kill target cells. Antitissue/cell antibodies: Antibodies may bind particularly to extracellular tissue antigens and the recruited leukocytes cause tissue injury, or antibodies may bind to cells (in this example, circulating pink cells) and promote depletion of these cells. Immune complexes: Complexes of antibodies and antigens may be shaped within the circulation and deposited in the walls of blood vessels, where the complexes induce inflammation. This classification is useful as a end result of distinct types of pathologic immune responses show different patterns of tissue injury and should differ in their tissue specificity. As a end result, the different immunologic mechanisms trigger issues with distinct clinical and pathologic options. However, immunologic ailments in humans are sometimes complex and attributable to combos of humoral and cell-mediated immune responses and multiple effector mechanisms. Antibodies in opposition to cellular or tissue antigens trigger ailments that specifically affect the cells or tissues where these antigens are current, so these ailments are sometimes organ-specific and never systemic. Therefore, immune complex�mediated diseases are inclined to be systemic and affect a quantity of tissues and organs, though some sites are notably prone, such as kidneys and joints. To prove that a illness is attributable to antibodies, one would wish to demonstrate that the lesions could be induced in a standard animal by the adoptive switch of immunoglobulin purified from the blood or affected tissues of people with the disease. An experiment of nature is occasionally seen in children of moms suffering from antibody-mediated illnesses.
Syndromes
- Vomiting
- Infection of the eye -- keratoconjunctivitis
- Eating a high-protein diet
- Congenital deficiency of factor IX (hemophilia B)
- Complete (has both external and internal openings)
- Pulmonary edema
- Joint pain or swelling
- Oily, foul-smelling, or bloody stools
40 mg citalopram with amex
These popliteal nodes receive lymph from tremendous cial vessels medicine encyclopedia generic citalopram 40mg with visa, which accompany the small saphenous vein symptoms miscarriage purchase citalopram 20mg with mastercard, and from deep areas of the leg and foot symptoms 2 days after ovulation generic citalopram 40mg otc. Deep fas cia of leg Deep fascia and the saphenous opening Fascia lata the outer layer of deep fascia in the decrease limb forms a thick "stocking-like" membrane, which covers the limb and lies beneath the super cial fascia. This deep fascia is especially thick in the thigh and gluteal area and is termed the fascia lata. The fascia lata is anchored superiorly to bone and soft tissues along a line of attachment that de nes the upper margin of the lower limb. Anterior s uperior iliac s pine Inguinal ligament Pectineal line Saphenous opening Pubic tubercle Femoral vein Fas cia lata Femoral triangle the femoral triangle is a wedge-shaped despair shaped by muscles within the upper thigh on the junction between the anterior belly wall and the lower limb. The medial border is the medial margin of the adductor longus muscle within the medial compartment of the thigh. The lateral margin is the medial margin of the sartorius muscle within the anterior compartment of the thigh. The oor of the triangle is fashioned medially by the pectineus and adductor longus muscle tissue within the medial compartment of the thigh and laterally by the iliopsoas muscle descending from the stomach. The apex of the femoral triangle factors inferiorly and is steady with a fascial canal (adductor canal), which descends medially down the thigh and posteriorly via an aperture within the lower finish of one of many largest of the adductor muscular tissues within the thigh (the adductor magnus muscle) to open into the popliteal fossa behind the knee. The femoral nerve, artery, and vein, and lymphatics cross between the abdomen and decrease limb underneath the inguinal ligament and within the femoral triangle. The Aorta Inferior vena cava Ps oas main Inguinal ligament Pubic s ymphys is Femoral triangle Pectineus mus cle Adductor longus mus cle Gracilis mus cle Adductor magnus mus cle Sartorius mus cle Inguinal ligament Femoral nerve Femoral s heath Lymphatics in femoral canal Femoral artery Femoral vein Pubic s ymphys is Adductor canal Adductor hiatus Great s aphenous vein Pubic bone Pubic s ymphys is. Regional anatomy � Gluteal area femoral artery and vein move inferiorly by way of the adductor canal and turn into the popliteal vessels behind the knee where they meet and are distributed with branches of the sciatic nerve, which descends through the posterior thigh from the gluteal area. From lateral to medial, main structures within the femoral triangle are the femoral nerve, the femoral artery, the femoral vein, and lymphatic vessels. Medial to the artery is the femoral vein and medial to the vein is the femoral canal, which incorporates lymphatics and lies immediately lateral to the pubic tubercle. Clinical app Vascular entry in the lower limb the femoral artery and vein are simply accessible within the femoral triangle. Many radiological procedures contain catheterization of the femoral artery or the femoral vein to acquire access to the contralateral decrease limb, the ipsilateral decrease limb, the vessels of the thorax and abdomen, and even the cerebral vessels. Cardiologists can also use the femoral artery to place catheters in vessels across the arch of the aorta and into the coronary arteries to carry out coronary angiography and angioplasty. Femoral sheath In the femoral triangle, the femoral artery and vein and the associated lymphatic vessels are surrounded by a funnelshaped sleeve of fascia (the femoral sheath). The sheath is steady superiorly with the transversalis fascia and iliacus fascia of the stomach and merges inferiorly with connective tissue related to the vessels. Each of the three constructions surrounded by the sheath is contained inside a separate fascial compartment within the sheath. The most medial compartment (the femoral canal) incorporates the lymphatic vessels and is conical in shape. The opening of this canal superiorly is potentially a weak point in the decrease abdomen and is the site for femoral hernias. Muscles in the area mainly abduct, lengthen, and laterally rotate the femur relative to the pelvic bone. The gluteal area communicates anteromedially with the pelvic cavity and perineum via the larger and lesser sciatic foramina, respectively. Sacrotuberous ligament Surface anatomy Finding the femoral artery in the femoral triangle the femoral artery descends into the thigh from the abdomen by passing underneath the inguinal ligament and into the femoral triangle. In the femoral triangle, its pulse is easily felt simply inferior to the inguinal ligament halfway between the pubic symphysis and the Anterior s uperior iliac s pine Inguinal ligament Femoral nerve Femoral artery Femoral vein Lymphatics pas s ing through femoral canal Pubic tubercle Medial margin of s artorius mus cle Pubic s ymphys is Medial margin of adductor longus mus cle Greater s ciatic foramen Sacros pinous ligament Quadrate tubercle Les s er s ciatic foramen Gluteal tuberos ity. An extra muscle on this group, the tensor fasciae latae, stabilizes the knee in extension by appearing on a specialised longitudinal band of deep fascia (the iliotibial tract) that passes down the lateral facet of the thigh to connect to the proximal finish of the tibia within the leg. It originates from between the anterior sacral foramina on the anterolateral floor of the sacrum and passes laterally and inferiorly through the greater sciatic foramen. Piriformis is a vital landmark because it divides the larger sciatic foramen into two areas, one above and one under the piriformis. The obturator internus muscle, like the piriformis muscle, is a muscle of the pelvic wall and of the gluteal region. The muscle bers of the obturator internus converge to form a tendon, which bends 90� around the ischium between the ischial spine and ischial tuberosity, and passes by way of the lesser sciatic foramen to enter the gluteal area. Gemellus superior and inferior (gemelli is Latin for "twins") are a pair of triangular muscular tissues associated with the higher and decrease margins of the obturator internus tendon. The gluteus medius and minimus muscle tissue abduct the pelvis over the stance limb at the hip joint and cut back pelvic drop over the other swing limb during walking. When standing on the affected limb, the pelvis severely drops over the swing limb. Positive ndings are sometimes found in patients with harm to the superior gluteal nerve. Damage to this nerve may happen with related pelvic fractures, house occupying lesions throughout the pelvis extending into the higher sciatic foramen and in some cases relating to hip surgery the place there has been Gluteus medius Gluteus minimus Greater s ciatic foramen above piriformis Piriformis mus cle Gemellus s uperior Contraction of gluteus minimus and medius on s tance s ide prevents exces s ive pelvic tilt throughout s wing phas e on oppos ite s ide Obturator internus Greater s ciatic foramen beneath piriformis Gemellus inferior Quadratus femoris B A 282. Regional anatomy � Gluteal region the superior gluteal nerve supplies branches to the gluteus minimus and medius muscles and terminates by innervating the tensor fasciae latae muscle. Typically through the stance section of the affected limb, the weakened abductor muscular tissues allow the pelvis to tilt inferiorly over the swing limb. The affected person compensates for the pelvic drop by lurching the trunk to the affected aspect to find a way to preserve the level of the pelvis all through the gait cycle. Sciatic nerve the sciatic nerve enters the gluteal region via the greater sciatic foramen inferior to the piriformis muscle. It descends within the airplane between the tremendous cial and deep group of gluteal area muscle tissue, crossing the posterior surfaces of rst the obturator internus and related gemellus muscles after which the quadratus femoris muscle. It lies just deep to the gluteus maximus at the midpoint between the ischial tuberosity and the larger trochanter. At the decrease margin of the quadratus femoris muscle, the sciatic nerve enters the posterior thigh. The sciatic nerve is the largest nerve in the physique and innervates all muscles within the posterior compartment of the thigh that ex the knee and all muscles that work the ankle and foot. Gluteus maximus is the biggest muscle within the gluteal area and overlies a lot of the different gluteal muscles. It is quadrangular in shape and has a broad origin from the bony pelvis and related ligaments and fascia. It is often described as being enclosed within two layers of the fascia lata, which covers the thigh and gluteal region. Laterally, the higher and tremendous cial lower components of the gluteus maximus insert into the iliotibial tract, which passes over the lateral floor of the greater trochanter and descends down the thigh and into the upper leg. Deep distal elements of the muscle connect to the elongate gluteal tuberosity of the proximal femur. Nerve to quadratus femoris the nerve to the quadratus femoris enters the gluteal region through the higher sciatic foramen inferior to the piriformis muscle and deep to the sciatic nerve. Unlike different nerves within the gluteal area, the nerve to the quadratus femoris lies anterior to the aircraft of the deep muscles. The nerve to the quadratus femoris descends alongside the ischium deep to the tendon of the obturator internus muscle and related gemellus muscular tissues to penetrate and innervate the quadratus femoris.
Citalopram 20mg low price
Here medications migraine headaches discount 40mg citalopram visa, the vessels have ascending and descending branches symptoms hepatitis c effective citalopram 20mg, which interconnect to form a longitudinal channel treatment 32 citalopram 20mg sale, which participates above in forming an anastomotic community of vessels around the hip and inferiorly anastomoses with branches of the popliteal artery behind the knee. Obturator artery the obturator artery originates as a branch of the internal iliac artery in the pelvic cavity and enters the medial compartment of thigh by way of the obturator canal. As it passes through the canal, it bifurcates into Lateral circum ex femoral artery the lateral circum ex femoral artery normally originates proximally from the lateral facet of the deep artery of thigh, but could arise instantly from the femoral artery. It passes deep to the sartorius and rectus femoris and divides into three terminal branches: One vessel (ascending branch) ascends laterally deep to the tensor fasciae latae muscle and connects with a branch of the medial circum ex femoral artery to form a channel, which circles the neck of the femur and provides the neck and head of the femur. One vessel (descending branch) descends deep to the rectus femoris, penetrates the vastus lateralis muscle and connects with a department of the popliteal artery near the knee. One vessel (transverse branch) passes laterally to pierce the vastus lateralis after which circles around the proximal shaft of femur to anastomose with branches from the medial femoral circum ex artery, the inferior gluteal artery, and the rst perforating artery to form the cruciate anastomosis across the hip. Medial circum ex femoral artery the medial circum ex femoral artery normally originates proximally from the posteromedial aspect of the deep artery of thigh, but could originate from the femoral artery. It passes medially around the shaft of femur, rst between the pectineus and iliopsoas and then between the obturator externus and adductor brevis muscle tissue. Near the margin of the adductor brevis, the vessel offers off a Obturator artery Acetabular department Artery of ligament of head of femur Ligament of head of femur Anterior department Obturator externus mus cle Pos terior branch. Vessels arising from the anterior and posterior branches supply adjoining muscles and anastomose with the inferior gluteal and medial circum ex femoral arteries. In addition, an acetabular vessel originates from the posterior branch, enters the hip joint by way of the acetabular notch, and contributes to the provision of the pinnacle of the femur. Great saphenous vein the good saphenous vein originates from a venous arch on the dorsal aspect of the foot and ascends along the medial facet of the lower limb to the proximal thigh. Here it passes via the saphenous opening within the deep fascia masking the anterior thigh to connect with the femoral vein in the femoral triangle. Clinical app Peripheral vascular illness Peripheral vascular illness is usually characterized by lowered blood ow to the legs. This dysfunction may be due to stenoses (narrowing) and/or occlusions (blockages) in the lower aorta, iliac, femoral, tibial, and bular vessels. Nerves There are three main nerves within the thigh, each related to one of the three compartments. Most patients with peripheral arterial illness have widespread arterial illness (including cardiovascular and cerebrovascular disease), which may be clinically asymptomatic. Some of these patients develop such severe ischemia that the viability of the limb is threatened (critical limb ischemia). Patients sometimes have a historical past of pain that develops within the calf muscles (usually associated with occlusions or narrowing within the femoral artery) or the buttocks (usually associated with occlusion or narrowing within the aorto-iliac segments). The patient rests and is ready to continue walking up to the identical distance till the ache recurs and stops walking as before. Pos terior department Pectineus mus cle Anterior cutaneous department Adductor longus mus cle Adductor magnus mus cle Gracilis mus cle Saphenous nerve Vas tus lateralis mus cle Rectus femoris mus cle Vas tus medialis mus cle Sartorius mus cle Acute on continual ischemia In some patients with chronic limb ischemia, an acute occasion blocks the vessels or reduces the blood provide to such a degree that the viability of the limb is threatened. Occasionally a leg might turn into acutely ischemic with no proof of underlying atheromatous illness. Patients with mitral valve disease and atrial brillation are vulnerable to embolic illness. Critical limb ischemia Critical limb ischemia happens when the blood provide to the limb is so poor that the viability of the limb is severely threatened, and in this case many patients develop gangrene, ulceration, and severe relaxation pain within the foot. These sufferers require urgent treatment, which can be in the type of surgical reconstruction, radiological angioplasty, and even amputation. Regional anatomy � Thigh is associated with the anterior compartment of thigh, the obturator nerve is related to the medial compartment of thigh, and the sciatic nerve is related to the posterior compartment of thigh. In the femoral triangle, the femoral nerve lies on the lateral aspect of the femoral artery and is outdoors the femoral sheath, which surrounds the vessels. Before coming into the thigh, the femoral nerve provides branches to the iliacus and pectineus muscle tissue. Immediately after passing beneath the inguinal ligament, the femoral nerve divides into anterior and posterior branches, which provide muscle tissue of the anterior compartment of thigh and skin on the anterior and medial features of the thigh and on the medial sides of the leg and foot. Rather, the saphenous nerve penetrates instantly via connective tissues close to the end of the canal to appear between the sartorius and gracilis muscular tissues on the medial aspect of the knee. Here the saphenous nerve penetrates deep fascia and continues down the medial aspect of the leg to the foot, and supplies pores and skin on the medial aspect of the knee, leg, and foot. Obturator nerve the obturator nerve is a branch of the lumbar plexus (spinal wire segments L2-L4) on the posterior belly wall. It descends within the psoas muscle, after which passes out of the medial margin of the psoas muscle to enter the pelvis. The obturator nerve continues alongside the lateral pelvic wall and then enters the medial compartment of thigh by passing via the obturator canal. It supplies many of the adductor muscular tissues and pores and skin on the medial aspect of the thigh. As the obturator nerve enters the thigh, it divides into two branches, an anterior department and a posterior branch, that are separated by the adductor brevis muscle: the posterior branch descends behind the adductor brevis muscle and on the anterior floor of the adductor magnus muscle, and supplies the obturator externus and adductor brevis muscular tissues and the a half of adductor magnus that attaches to the linea aspera. The anterior department descends on the anterior surface of the adductor brevis muscle and is behind the pectineus and adductor longus muscles-it supplies branches to the adductor longus, gracilis, and adductor brevis muscle tissue, and often contributes to the availability of the pectineus muscle, and cutaneous branches innervate the pores and skin on the medial aspect of the thigh. Ps oas and iliacus mus cles Obturator nerve Obturator externus mus cle Pos terior department Anterior branch Pectineus mus cle Adductor brevis mus cle Cutaneous department Adductor longus mus cle Branch to adductor magnus from pos terior branch Gracilis mus cle Adductor magnus mus cle Sciatic nerve the sciatic nerve is a department of the lumbosacral plexus (spinal twine segments L4-S3) and descends into the posterior compartment of thigh from the gluteal region. It innervates all muscle tissue in the posterior compartment of thigh and then its branches proceed into the leg and foot. In the posterior compartment of thigh, the sciatic nerve lies on the adductor magnus muscle and is crossed by the lengthy head of biceps femoris muscle. Proximal to the knee, and generally throughout the pelvis, the sciatic nerve divides into its two terminal branches: the tibial nerve and the widespread bular nerve. These nerves travel vertically down the thigh and enter the popliteal fossa posterior to the knee. The tibial nerve provides branches to all muscular tissues within the posterior compartment of thigh (long head of biceps. The detailed movements of the knee joint are complex, however mainly the joint is a hinge joint that enables primarily exion and extension. The joint consists of: the articulation between the femur and tibia, which is weight bearing, and the articulation between the patella and the femur, which allows the pull of the quadriceps femoris muscle to be directed anteriorly over the knee to the tibia without tendon wear. Articular surfaces the articular surfaces of the bones that contribute to the knee joint are lined by hyaline cartilage. The major surfaces involved embody: the two femoral condyles, and the adjoining surfaces of the superior facet of the tibial condyles. The surfaces of the femoral condyles that articulate with the tibia in exion of the knee are curved or spherical, whereas the surfaces that articulate in full extension are at. The articular surfaces between the femur and patella are the V-shaped trench on the anterior floor of the distal end of the femur the place the 2 condyles be a part of and the adjacent surfaces on the posterior side of the patella. The joint surfaces are all enclosed within a single articular cavity, as are the intra-articular menisci between the femoral and tibial condyles.
Purchase citalopram 20mg overnight delivery
For example medications 5 rights cheap 20mg citalopram with visa, the physical association of two completely different proteins in the membrane of a lymphocyte could be established by immunoprecipitating a membrane extract by use of an antibody particular for one of the proteins and probing a Western blot of the immunoprecipitate using an antibody specific for the second protein that may have been co-immunoprecipitated together with the primary protein medicine zebra discount citalopram 40mg overnight delivery. Identification and Purification of Proteins Antibodies can be used to establish and characterize proteins and to purify particular proteins from mixtures symptoms definition citalopram 40 mg free shipping. Two commonly used strategies to establish and purify proteins are immunoprecipitation and immuno-affinity chromatography. Western blotting is a broadly used method to decide the presence and size of a protein in a biologic sample. Immunoprecipitation and Immuno-Affinity Chromatography Immunoprecipitation is a way during which an antibody specific for one protein antigen in a mixture of proteins is used to identify this particular antigen. The antibody is often added to a protein combination (usually a detergent lysate of specific cells), and staphylococcal protein A (or protein G) covalently attached to agarose beads is added to the combination. The Fab portions of the antibody bind to the goal protein, and the Fc portion of the antibody is captured by the protein A or protein G on the beads. Proteins may be detected after electrophoresis by staining the polyacrylamide gel with a protein stain or by a Western blot analysis (described later). Immuno-affinity chromatography, a variant of affinity chromatography, is a purification method that depends on antibodies hooked up to an insoluble support to purify antigens from an answer. A, A specific antigen could be purified from a combination of antigens in serum or other options by adding antibodies specific to the antigen which are certain to insoluble beads. Unbound antigens are then washed away, and the desired antigen is recovered by changing the pH or ionic power of the answer so that the affinity of antibody-antigen binding is lowered. Immunoprecipitation can be utilized as a way of purification, as a means of quantification, or as a method of identification of an antigen. Antigens purified by immunoprecipitation are often analyzed by sodium dodecyl sulfate�polyacrylamide gel electrophoresis. B, Affinity chromatography is based on the same principle as immunoprecipitation, except that the antibody is mounted to an insoluble matrix or beads, often in a column. The technique is often used to isolate soluble antigens (shown) or antibodies particular for an immobilized antigen. Labeling and Detection of Antigens in Cells and Tissues Antibodies specific for antigens expressed on or particularly cell types are generally used to identify these cells in tissues or cell suspensions and to separate these cells from combined populations. In these strategies, the antibody can be radiolabeled, enzyme linked, or, mostly, fluorescently labeled, and a detection system is used that can identify the certain antibody. Antibodies attached to magnetic beads can be utilized to bodily isolate cells expressing specific antigens. Flow Cytometry the tissue lineage, maturation stage, or activation status of a cell can typically be decided by analyzing the cell floor or intracellular expression of different molecules. This is commonly carried out by staining the cell with fluorescently labeled probes that are specific for these molecules and measuring the amount of fluorescence emitted by the cell. The incident laser beam is of a designated wavelength, and the sunshine that emerges from the pattern is analyzed for forward and aspect scatter in addition to fluorescent gentle of two or more wavelengths that depend upon the fluorochrome labels attached to the antibodies. The separation depicted here relies on two antigenic markers (two-color sorting). Modern instruments can routinely analyze and separate cell populations on the basis of three or more different-colored probes. Suspensions of cells are incubated with fluorescently labeled probes, and the amount of probe bound by every cell in the population is measured by passing the cells separately through a fluorimeter with a laser-generated incident beam. The relative quantities of a specific molecule on totally different cell populations may be compared by staining each inhabitants with the identical probe and determining the amount of fluorescence emitted. In preparation for circulate cytometric analysis, cell suspensions are stained with the fluorescent probes of alternative. Most typically, these probes are fluorochrome-labeled antibodies specific for a cell surface molecule. Alternatively, cytoplasmic molecules could be stained by quickly permeabilizing cells and allowing the labeled antibodies to enter by way of the plasma membrane. In addition to antibodies, various fluorescent indicators of cytoplasmic ion concentrations and reduction-oxidation potential could be detected by move cytometry. Apoptotic cells could be identified with fluorescent probes, such as annexin V, that bind to abnormally exposed phospholipids on the surface of the dying cells. Modern move cytometers can routinely detect three or more different-colored fluorescent alerts, each attached to a unique antibody or different probe. This technique permits simultaneous analysis of the expression of many various combinations of molecules by a cell. In addition to detecting fluorescent signals, circulate cytometers additionally measure the ahead and facet light-scattering properties of cells, which mirror cell size and inner complexity, respectively. For instance, in contrast with lymphocytes, neutrophils trigger higher aspect scatter due to their cytoplasmic granules, and monocytes cause higher ahead scatter because of their measurement. A newly developed antibody-based technology known as mass cytometry combines the single-cell circulate expertise of move cytometers with mass spectrometry. Antibodies particular for molecules of interest are labeled with any certainly one of a lot of heavy metals, utilizing a unique steel for every antibody specificity. Unlike fluorescence labels, many different heavy steel labels can be resolved by mass spectrometry without overlap, permitting for the detection of as many as a hundred completely different molecules on a single cell. These beads are mixed with the check resolution that accommodates multiple cytokines, such as serum or supernatants of lymphocyte cultures. Each cytokine will bind solely to beads of one specific size and fluorescence intensity. The beads are simultaneously analyzed by a two-laser flow-based detection instrument. Standard options with recognized concentrations of the cytokines are used to calibrate the outcomes. This method is completed by differentially deflecting the cells with electromagnetic fields whose power and course are diversified according to the measured intensity of the fluorescent signal. The cells may be labeled with fluorescently tagged antibodies ex vivo, or, within the case of experimental animal studies, labeling may be accomplished in vivo by expression of transgenes that encode fluorescent proteins, similar to green fluorescent protein. These "immunomagnetic reagents" will bind to sure cells, depending on the specificity of the antibody used, and the bound cells can then be pulled out of suspension by a strong magnet. Immunofluorescence and Immunohistochemistry Antibodies can be utilized to determine the anatomic distribution of an antigen within a tissue or within compartments of a cell. In the earliest model of this technique, referred to as immunofluorescence, the antibody was labeled with a fluorescent dye and allowed to bind to a monolayer of cells or to a frozen part of a tissue. The stained cells or tissues have been examined with a fluorescence microscope to locate the antibody. This downside has been overcome by new technologies including confocal microscopy, which makes use of optical sectioning know-how to filter out unfocused fluorescent gentle, and two-photon microscopy, which prevents outof-focus light from forming. Alternatively, antibodies could additionally be coupled to enzymes that convert colorless substrates to coloured insoluble substances that precipitate at Cytokine Bead Assays In these assays, the focus of many alternative cytokines in a single resolution could be decided concurrently. A conventional mild microscope might then be used to localize the antibody in a stained cell or tissue. The most typical variant of this technique uses the enzyme horseradish peroxidase, and the strategy is often referred to because the immunoperoxidase technique.
Order citalopram 20mg free shipping
Between the posterior talar articular surface symptoms week by week buy 20mg citalopram visa, which articulates with the body of the talus and the other two articular surfaces medications errors cheap 20mg citalopram mastercard, which articulate with the pinnacle of the talus medications 319 discount citalopram 40mg on line, is a deep groove (the calcaneal sulcus;. Clinical app Achilles tendon rupture Rupture of the Achilles tendon is usually associated to sudden or direct trauma. In addition, there are certain circumstances that will predispose the tendon to rupture. Among these situations are tendinopathy (due to overuse, or to age-related degenerative changes) and previous Achilles tendon interventions similar to injections of pharmaceuticals and using sure antibiotics (quinolone group). Intermediate tarsal bone the intermediate tarsal bone on the medial side of the foot is the navicular (boat shaped). This bone articulates behind with the talus and articulates in entrance and on the lateral facet with the distal group of tarsal bones. One distinctive feature of the navicular is a outstanding rounded tuberosity for the attachment of the tibialis posterior tendon, which projects inferiorly on the medial aspect of the plantar surface of the bone. Distal group 318 From lateral to medial, the distal group of tarsal bones consists of. Three cuneiforms (Latin for "wedge")-the lateral, intermediate, and medial cuneiform bones, in addition to articulating with one another, articulate posteriorly with the navicular bone and anteriorly with the bases of the medial three metatarsals. The lateral side of the base of metatarsal V has a outstanding tuberosity, which projects posteriorly and is the attachment site for the tendon of the bularis brevis muscle. Each metatarsal has a head on the distal finish, an elongate shaft in the middle, and a proximal base. The head of every metatarsal articulates with the proximal phalanx of a toe and the bottom articulates with one or more of the distal group of tarsal bones. Each toe has three phalanges (proximal, middle, and distal), except for the great toe, which has solely two (proximal and distal). Each phalanx consists of a base, a shaft, and a distal head: the base of each proximal phalanx articulates with the top of the associated metatarsal. The head of every distal phalanx is nonarticular and attened right into a crescent-shaped plantar tuberosity under the plantar pad at the end of the digit. In each toe, the total size of the phalanges combined is way shorter than the length of the related metatarsal. Imaging app Visualizing the bones of the foot Medial Metatars als cuneiform Navicular Talus Tibia Fibula. The ankle joint is synovial in kind and includes the talus of the foot and the tibia and bula of the leg. The ankle joint mainly permits hingelike dorsi exion and plantar exion of the foot on the leg. The distal end of the bula is rmly anchored to the bigger distal end of the tibia by robust ligaments. Together, the bula and tibia create a deep bracket-shaped socket for the upper expanded a half of the body of the talus: the roof of the socket is formed by the inferior surface of the distal end of the tibia. The longer lateral aspect of the socket is formed by the lateral malleolus of the bula. The articular a half of the talus is formed like a brief half cylinder tipped onto its at aspect with one end facing lateral and the other end going through medial. The curved upper floor of the half cylinder and the two ends are covered by hyaline cartilage and t into the bracket-shaped socket formed by the distal ends of the tibia and bula. As a result, the bone ts tighter into its socket when the foot is dorsi exed and the broader surface of the talus moves into the ankle joint than when the foot is plantar exed and the narrower a part of the talus is in the joint. The articular cavity is enclosed by a synovial membrane, which attaches around the margins of the articular surfaces, and by a brous membrane, which covers the synovial membrane and can additionally be hooked up to the adjoining bones. The tibiocalcaneal half, which is more central, attaches to the sustentaculum tali of the calcaneus bone. The posterior tibiotalar part attaches to the medial facet and medial tubercle of the talus. The fourth part (the anterior tibiotalar part) is deep to the tibionavicular and tibiocalcaneal parts of the medial ligament and attaches to the medial floor of the talus. Its apex is hooked up above to the medial malleolus and its broad base is attached beneath to a line that extends from the tuberosity of the navicular bone in entrance to the medial tubercle of the talus behind. The medial ligament is subdivided into four components based mostly on the inferior factors of attachment. Fibrous cubonavicular joint Lateral ligament the lateral ligament of the ankle consists of three separate ligaments, the anterior talo bular ligament, the posterior talo bular ligament, and the calcaneo bular ligament. The posterior talo bular ligament runs horizontally backward and medially from the malleolar fossa on the medial side of the lateral malleolus to the posterior process of the talus. The calcaneo bular ligament is connected above to the malleolar fossa on the posteromedial aspect of the lateral malleolus and passes posteroinferiorly to attach beneath to a tubercle on the lateral surface of the calcaneus. Navicular Calcaneocuboid joint Talocalcaneonavicular joint Trans ve rs e tars al jo int Cuboid Talus Subtalar joint Calcaneus Intertarsal joints the quite a few synovial joints between the person tarsal bones primarily invert, evert, supinate, and pronate the foot. Pronation is rotating the front of the foot laterally relative to the again of the foot, and supination is the reverse motion. Coronal view of ankle joint exhibiting posterior talo bular and calcaneo bular ligaments. The main joints at which actions happen include the subtalar, talocalcaneonavicular, and calcaneocuboid joints. The talocalcaneonavicular and calcaneocuboid joints collectively kind what is often referred to as the transverse tarsal joint. Intertarsal joints between the cuneiforms and between the cuneiforms and the navicular permit solely restricted movement. Interos s eous talocalcaneal ligament 6 Talus Subtalar joint Calcaneus Clinical app Ankle injuries the anatomy of the ankle joint is complicated. However, from a scientific perspective it could be thought to be a bro-osseous ring oriented within the coronal aircraft. The upper part of the ring is fashioned by the distal ends of the bula and tibia, the distal joint between the tibia and bula, the tibio bular ligaments, and the ankle joint itself. The sides of the ring are formed by the ligaments that connect the medial malleolus and lateral malleolus to the adjacent tarsal bones. The medial (deltoid) ligament consists of the anterior tibiotalar, posterior tibiotalar, tibiocalcaneal, and tibionavicular components. The lateral ligament consists of the anterior talo bular ligament, calcaneo bular ligament, and the posterior talo bular ligament. In this harm, the anterior talo bular and calcaneo bular parts of the lateral ligament are disrupted. These buildings, once disrupted, enable the ankle to invert typically producing a fracture of the medial malleolus or a partial tear to the medial (deltoid) ligament. The subtalar joint permits gliding and rotation, that are involved in inversion and eversion of the foot. Lateral, medial, posterior, and interosseous talocalcaneal ligaments stabilize the joint.
Goji Berry (Lycium). Citalopram.
- Dosing considerations for Lycium.
- Are there any interactions with medications?
- Diabetes, high blood pressure, fever, malaria, cancer, blood circulation problems, sexual problems (impotence), dizziness, ringing in the ears (tinnitus), and many other conditions.
- How does Lycium work?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96984
Buy citalopram 20 mg mastercard
IgA is the primary immunoglobulin in secretions medicine zoloft order 20mg citalopram amex, significantly of the gastrointestinal tract 911 treatment center citalopram 20mg cheap. Some essential biochemical and organic correct ties of the three major immunoglobulin subclasses are summa rized in Table 9 medications you can take during pregnancy 40 mg citalopram fast delivery. Each molecule is made up of two mild (k or l) (blue areas) and two heavy (purple) chains, and every chain is made up of variable (V) and constant (C) portions, the V portions including the antigen binding site. IgG antibody can be broken into a relentless Fc fragment and two extremely variable Fab fragments. IgG Molecular weight Normal serum stage (g/L) Present in Complement fixation Placental switch Heavy chain 140 000 6. However, additionally they have a significant position in the pathogenesis of a variety of haematological problems. Secretion of a specific immunoglobulin from a monoclonal inhabitants of lymphocytes or plasma cells causes paraproteinaemia (see p. Bence�Jones protein discovered within the urine in some circumstances of myeloma consists of a monoclonal secretion of sunshine chains or lightchain fragments (either k or l). Immu noglobulins could bind to blood cells in quite a lot of immune issues and trigger their agglutination. Antigen�receptor gene rearrangements Immunoglobulin gene rearrangements the immunoglobulin heavychain and k and l lightchain genes occur on chromosomes 14, 2 and 22, respectively. In the germline state, the heavychain gene consists of separate seg ments for variable (V), variety (D), becoming a member of (J) and fixed (C) areas. In cells not commit ted to immunoglobulin synthesis these gene segments stay in their separate germline state. Diversity is introduced by the variability of which V section joins with which D and with which J segment. Further mutation of the V region genes happens within the germinal centres of secondary lymphoid tissues (called somatic mutation) (see below). These acknowledge certain heptamer and nonamerconserved sequences flanking the various gene segments. Mistakes in recombinase exercise play an necessary half in the chromosome translocations of B or Tcell malignancy. The class of immunoglobulin is dependent upon which of the nine constant regions (1m, 1d, 4g, 2a, 1e) is used. The most plentiful and pivotal protein is C3, which is current in plasma at a level of approximately 1. The early (opsonizing) phases resulting in coating of the cells with C3b can happen by two completely different pathways: 1. The alternate pathway, which is more speedy and activated by IgA, endotoxin (from Gramnegative bacteria) and oth er components. Macrophages and neutrophils have C3b receptors and so they phagocytose C3bcoated cells. C3b is degraded to C3d detected in the direct antiglobulin take a look at utilizing an anticom plement agent (p. The complement pathway additionally generates the biologically energetic fragments C3a and C5a which act instantly on phagocytes to stimulate the respiratory burst (p. Both might set off anaphylaxis by launch of mediators from tissue mast cells and basophils, which cause vasodilatation and increased permeability. The immune response One of probably the most hanging features of the immune system is its capability to produce a extremely specific response. For both T and B cells this specificity is achieved by the presence of a particu lar receptor on the lymphocyte floor. Each of those lymphocytes has a receptor that shows variations in structure from that of another lymphocyte. At this stage, lymphocytes could turn into effector cells (such as plasma cells or cytotoxic T cells) or memory cells. In the classic pathway, the convertase is the most important (b) part of C4 and C2 (C4b2b). Antigenspecific immune responses are generated in secondary lymphoid organs and begin when antigen is carried right into a lymph node. B cells acknowledge antigen by way of their surface immunoglobulin and though most antibody responses require help from antigen specific T cells, some antigens such as polysaccharides can lead to Tcell impartial B cell antibody manufacturing. In the fol licle, germinal centres come up on account of persevering with response to antigenic stimulation. B cells activated by antigen migrate from the T zone to the follicle the place they endure large proliferation. Cells enter the darkish zone as centroblasts and accumulate mutations of their immunoglobulin V genes. Only these cells that may interact with antigen on follicular dendritic cells and receive signals from antigenspecific T cells. Proliferating B cells transfer to the darkish zone of the germinal centre as centroblasts where they undergo somatic mutation of their immunoglobulin variableregion genes. Glandular fever is a general term for a disease character ized by fever, sore throat, lymphadenopathy and atypical lymphocytes within the blood. Clinical options the majority of patients are between the ages of 15 and forty years. A prodromal period of some days occurs with lethargy, malaise, headaches, stiff neck and a dry cough. In established disease the following features may be found: 1 Bilateral cervical lymphadenopathy is present in 75% of circumstances. These T cells are variable in look however most have nuclear and cytoplasmic options much like these seen during reactive lymphocyte transformation. The best number of atypi cal lymphocytes are normally found between the seventh and tenth day of the sickness. Heterophile antibodies Heterophile antibodies in opposition to sheep or horse pink cells could additionally be discovered in the serum at excessive titres. Modern slide screening checks, such because the monospot test, use formalinized horse pink cells to test for the IgM antibodies which agglutinate the cells. Chapter 9: White cells: lymphocytes / 113 titres happen through the second and third week and the antibody persists in most patients for six weeks. Haematological abnormalities Haematological abnormalities other than the atypical lym phocytosis are frequent. Thrombocytopenia is frequent and an autoimmune thrombocytopenic purpura happens in a smaller number of patients. Treatment In the nice majority of patients only symptomatic therapy is required. Patients characteristically develop an erythematous rash if given ampicillin remedy. However, convalescence could also be slow and related to extreme malaise and lethargy. Lymphopenia Lymphopenia could occur in extreme bone marrow failure, with corticosteroid and other immunosuppressive remedy, in Hodgkin lymphoma and with widespread irradiation.
20mg citalopram fast delivery
Mononuclear phagocytes flow into within the blood in an incompletely differentiated form known as monocytes treatment west nile virus citalopram 40mg low price, and after they settle in tissues treatment sinus infection citalopram 20 mg cheap, they mature into macrophages medications mobic buy 40mg citalopram amex. Mucosa-associated lymphoid tissues include intraepithelial lymphocytes, mainly T 508 Glossary cells, and organized collections of lymphocytes, usually rich in B cells, under mucosal epithelia, similar to Peyer patches within the gut or pharyngeal tonsils. Mucosal immune system A a part of the immune system that responds to and protects in opposition to microbes that enter the body via mucosal surfaces, such as the gastrointestinal and respiratory tracts, but in addition maintains tolerance to commensal organisms that live on the outside of the mucosal epithelium. The mucosal immune system is composed of organized mucosaassociated lymphoid tissues, corresponding to Peyer patches, as well as diffusely distributed cells throughout the lamina propria. Multiple myeloma A malignant tumor of antibodyproducing B cells that always secretes Igs or components of Ig molecules. The monoclonal antibodies produced by multiple myelomas have been critical for early biochemical analyses of antibody structure. Mycobacterium A genus of aerobic bacteria, many species of which might survive within phagocytes and cause illness. The principal host protection against mycobacteria such as Mycobacterium tuberculosis is cellmediated immunity. Myeloid-derived suppressor cells A heterogeneous group of immature myeloid precursors that suppress anti-tumor immune responses and are present in lymphoid tissues, blood, or tumors of tumor-bearing animals and most cancers sufferers. Naive lymphocyte A mature B or T lymphocyte that has not beforehand encountered antigen. Naive lymphocytes have surface markers and recirculation patterns which are distinct from these of beforehand activated lymphocytes. Normal individuals contain natural antibodies without any evidence of an infection, and these antibodies serve as a preformed defense mechanism towards microbes that succeed in penetrating epithelial limitations. Negative selection the process by which growing lymphocytes that specific self-reactive antigen receptors are eliminated, thereby contributing to the maintenance of self-tolerance. Neoepitopes encoded by mutated proteins are the main inducers of tumor-specific T cell responses. Neonatal Fc receptor (FcRn) An IgG-specific Fc receptor that mediates the transport of maternal IgG across the placenta and the neonatal intestinal epithelium and, in adults, promotes the lengthy half-life of IgG molecules within the blood by protecting them from catabolism by phagocytes and endothelial cells. Neonatal immunity Passive humoral immunity to infections in mammals within the first months of life, earlier than full development of the immune system. Neonatal immunity is mediated by maternally produced antibodies transported throughout the placenta into the fetal circulation earlier than delivery or derived from ingested milk and transported throughout the gut epithelium. Nitric oxide A molecule with a broad range of activities that in macrophages capabilities as a potent microbicidal agent to kill ingested organisms. Nitric oxide synthase A member of a household of enzymes that synthesize the vasoactive and microbicidal Glossary 509 compound nitric oxide from L-arginine. Macrophages categorical an inducible form of this enzyme on activation by various microbial or cytokine stimuli. Notch-1 signaling is required for commitment of growing T cell precursors to the T cell lineage. Nude mouse A strain of mice that lacks growth of the thymus, and due to this fact T lymphocytes, as nicely as hair follicles. Nude mice have been used experimentally to outline the position of T lymphocytes in immunity and disease. Oncofetal antigen Proteins which might be expressed at high levels on some types of cancer cells and in regular developing fetal (but not adult) tissues. Antibodies specific for these proteins are sometimes utilized in histopathologic identification of tumors or to monitor the progression of tumor progress in sufferers. Opsonin A molecule that turns into hooked up to the floor of a microbe and can be recognized by floor receptors of neutrophils and macrophages and that increases the effectivity of phagocytosis of the microbe. Opsonization the method of attaching opsonins, corresponding to IgG or complement fragments, to microbial surfaces to goal the microbes for phagocytosis. Oral tolerance the suppression of systemic humoral and cell-mediated immune responses to an antigen after the oral administration of that antigen because of anergy of antigen-specific T cells or the manufacturing of immunosuppressive cytokines corresponding to reworking progress factor-. Oral tolerance is a potential mechanism for prevention of immune responses to food antigens and to bacteria that usually reside as commensals in the intestinal lumen. Paracrine factor A molecule that acts on cells in proximity to the cell that produces the issue. The recipient of such a switch can turn into immune to the antigen without ever having been exposed to or having responded to the antigen. An instance of passive immunity is the transfer of human sera containing antibodies specific for sure microbial toxins or snake venom to a beforehand unimmunized particular person. Multiple mechanisms may contribute to pathogenicity, including production of poisons, stimulation of host inflammatory responses, and perturbation of host cell metabolism. Pentraxins A family of plasma proteins that comprise five equivalent globular subunits; consists of the acutephase reactant C-reactive protein. The cleft is composed of paired helices resting on a floor made up of an eight-stranded -pleated sheet. Peripheral lymphoid organs and tissues Organized collections of lymphocytes and accessory cells, including the spleen, lymph nodes, and mucosa-associated lymphoid tissues, by which adaptive immune responses are initiated. Peripheral tolerance Unresponsiveness to self antigens which are present in peripheral tissues and never normally within the generative lymphoid organs. Peripheral tolerance is induced by the popularity of antigens with out enough ranges of the costimulators required for lymphocyte activation or by persistent and repeated stimulation by these self antigens. Phagocytosis the process by which certain cells of the innate immune system, together with macrophages and neutrophils, engulf giant particles (>0. The cell surrounds the particle with extensions of its plasma membrane by an energy- and cytoskeleton-dependent process; this process results in the formation of an intracellular vesicle called a phagosome, which incorporates the ingested particle. Phagosome A membrane-bound intracellular vesicle that incorporates microbes or particulate materials ingested from the extracellular surroundings. They fuse with other vesicular buildings corresponding to lysosomes, resulting in enzymatic degradation of the ingested materials. Phosphatase (protein phosphatase) An enzyme that removes phosphate groups from the facet chains of sure amino acid residues of proteins. Some protein phosphatases could also be particular for phosphotyrosine residues and others for phosphoserine and phosphothreonine residues. Plasmablast Circulating antibody-secreting cells which would possibly be precursors of the plasma cells that reside in the bone marrow and different tissues. Plasma cell A terminally differentiated antibodysecreting B lymphocyte with a attribute histologic look, including an oval form, eccentric nucleus, and perinuclear halo. Polyclonal activators Agents which are able to activating many clones of lymphocytes, no matter their antigen specificities. Poly-Ig receptor An Fc receptor expressed by mucosal epithelial cells that mediates the transport of IgA and IgM by way of the epithelial cells into the intestinal lumen. Polymorphism the existence of two or extra alternative forms, or variants, of a gene which may be current at steady frequencies in a population.
Buy 20mg citalopram overnight delivery
The plasma membrane invaginates into the platelet interior to kind an open membrane (canalicular) system which provides a big reactive floor to which the plasma coagulation proteins could also be selectively absorbed medications quetiapine fumarate generic citalopram 20mg with amex. Platelets are additionally rich in signalling and cytoskeletal proteins treatment ringworm order citalopram 20 mg line, which help the fast switch from quiescence to activation that follows vessel damage symptoms after miscarriage cheap citalopram 40mg mastercard. During the discharge reaction described under, the contents of the granules are discharged into the open canalicular system. Platelet function the principle perform of platelets is the formation of mechanical plugs in the course of the haemostatic response to vascular damage. In the absence of platelets, spontaneous leakage of blood by way of small vessels may happen. There are three main platelet functions: adhesion, aggregation and release reactions and amplification. It is a large glycoprotein, with multimers made up on common of 2�50 dimeric subunits. The majority is continuously secreted and a minority is saved in Weibel� Palade bodies. Platelet release response and amplification Primary activation by various agonists induces intracellular signalling, leading to the discharge of granule contents. It is a potent inhibitor of platelet aggregation and prevents their deposition on regular vascular endothelium. Platelet procoagulant exercise After platelet aggregation and release, the exposed membrane phospholipid (platelet issue 3) is out there for two reactions within the coagulation cascade. The phospholipid floor forms a perfect template for the essential concentration and orientation of those proteins. This results in further binding to von Willebrand factor and so results in additional platelet adhesion to the subendothelium. Blood coagulation the coagulation cascade Blood coagulation in vivo involves a organic amplification system in which comparatively few initiation substances sequentially activate by proteolysis a cascade of circulating precursor proteins (the coagulation factor enzymes) which culminates within the technology of thrombin; this, in turn, converts soluble plasma fibrinogen into fibrin. Fibrin enmeshes the platelet aggregates at the websites of vascular harm and converts the unstable primary platelet plugs to firm, definitive and steady haemostatic plugs. The operation of this enzyme cascade requires local concentration of circulating coagulation factors at the site of harm. Surfacemediated reactions happen on exposed collagen, platelet phospholipid and tissue factor. With the exception of fibrinogen, which is the fibrin clot subunit, the coagulation factors are both enzyme precursors or cofactors (Table 24. Coagulation in vivo the technology of thrombin in vivo is a fancy network of amplification and unfavorable feedback loops to ensure a localized and restricted manufacturing. The generation of thrombin is Chapter 24: Platelets, blood coagulation and haemostasis / 271 Table 24. The era of thrombin following vascular harm occurs in two waves of very different magnitude. During the preliminary part small amounts of thrombin are generated (picomolar concentrations). It is expressed on fibroblasts and small muscular tissues of the vessel wall and in the blood stream on microparticles, and on different nonvascular cells. The factor Xa, in the absence of its cofactor, forms small quantities of thrombin from prothrombin. The technology of thrombin from prothrombin by the motion of Xa�Va complicated leads to fibrin formation. Importantly, the small quantities of thrombin generated serve to tremendously amplify coagulation. Thrombin hydrolyses fibrinogen, releasing fibrinopeptides A and B to form fibrin monomers. Fibrin monomers hyperlink spontaneously by hydrogen bonds to type a loose insoluble fibrin polymer. After cleavage by thrombin of small fibrinopeptides A and B from the and chains, fibrin monomer consists of three paired, and chains which rapidly polymerise. This cell provides the basement membrane that normally separates collagen, elastin and fibronectin of the subendothelial connective tissue from the circulating blood. Loss of or injury to the endothelium leads to each haemorrhage and activation of the haemostatic mechanism. The reduced blood flow allows contact activation of platelets and coagulation components. Endothelial cells produce substances that may initiate coagulation, trigger vasodilatation, inhibit platelet aggregation or haemostasis, or activate fibrinolysis. This continuing platelet aggregation promotes the growth of the haemostatic plug, which quickly covers the exposed connective tissue. The unstable major haemostatic plug produced by these platelet reactions in the first minute or so following harm is often adequate to present short-term management of bleeding. Stabilization of the platelet plug by fibrin Definitive haemostasis is achieved when fibrin, shaped by blood coagulation, is added to the platelet mass and by plateletinduced clot retraction/compaction. Platelet aggregation and launch reactions accelerate the coagulation course of by offering ample membrane phospholipid. The fibrin element of the haemostatic plug increases because the fused platelets fully degranulate and autolyse, and after a couple of hours the entire haemostatic plug is remodeled right into a solid mass of cross linked fibrin. Chapter 24: Platelets, blood coagulation and haemostasis / 275 Coagulation factor inhibitors It is important that the effect of thrombin is proscribed to the location of damage. There can be direct inactivation of thrombin and other serine protease elements by different circulating inhibitors, of which antithrombin is probably the most potent. The motion of protein C is enhanced by another vitamin Kdependent protein, S, which binds protein C to the platelet surface. An endothelial protein C receptor localizes protein C to the endothelial floor, selling protein C activation by the thrombin�thrombomodulin complex. As with different serine proteases, activated protein C is topic to inactivation by serum protease inactivators (serpins). Blood move At the periphery of a broken space of tissue, blood flow quickly achieves dilution and dispersal of activated components before fibrin formation has occurred. Activated elements are destroyed by liver parenchymal cells and particulate matter is removed by liver Kupffer cells and different reticuloendothelial cells. Fibrinolysis Fibrinolysis (like coagulation) is a normal haemostatic response to vascular injury. Plasminogen, a proenzyme in blood and tissue fluid, is transformed to the serine protease plasmin by activators either from the vessel wall (intrinsic activation) or from the tissues (extrinsic activation). Plasmin era on the web site of harm limits the extent of the evolving thrombus. The split products of fibrinolysis are additionally aggressive inhibitors of thrombin and fibrin polymerization. Protein S is a cofactor that facilitates binding of activated protein C to the platelet floor. Cleavage of peptide bonds in fibrin and fibrinogen produces a wide range of cut up (degradation) merchandise. Large amounts of the smallest fragments can be detected within the plasma of patients with disseminated intravascular coagulation (see p.
20mg citalopram with amex
Mesenteric lymph nodes gather lymph-borne antigens from the small and large intestines and are websites of differentiation of effector and regulatory lymphocytes that house back to the lamina propria medications on nclex rn cheap citalopram 20 mg with visa. The cells that differentiate within the mesenteric lymph nodes in response to bowel wall invasion by pathogens or commensals usually house to the lamina propria (discussed later) medicine to treat uti citalopram 20mg low cost. Lingual and palatine tonsils are unencapsulated lymphoid constructions situated beneath stratified squamous epithelial mucosa within the base of the tongue and oropharynx 6mp medications effective 40mg citalopram, respectively, and are websites of immune responses to microbes within the oral cavity. The bulk of the tonsillar tissue consists of lymphoid follicles, usually with prominent germinal centers. There are numerous narrow and deep invaginations of the floor squamous epithelium, referred to as crypts, which grow into the tonsillar follicular tissue. The lingual and palatine tonsils respond to infections of the epithelial mucosa by vital enlargement and vigorous, primarily IgA, antibody responses. Typical infections which would possibly be related to tonsillar enlargement, normally in kids, are caused by streptococci and the Epstein-Barr virus. The functions of the gastrointestinal immune system rely upon a large number of T cells and antibody-secreting cells which might be in a place to recirculate back into the lamina propria and reply quickly to pathogens. The lamina propria incorporates diffusely distributed effector lymphocytes, dendritic cells, and macrophages and is the site of the effector part of gastrointestinal adaptive immune responses. In this location, T cells can respond to invading pathogens, and B cells can secrete antibodies that are transported into the lumen and neutralize pathogens earlier than they invade. Humoral Immunity within the Gastrointestinal Tract the main perform of humoral immunity within the gastrointestinal tract is to neutralize luminal microbes, and this perform is mediated mainly by IgA produced in the lamina propria and transported throughout the mucosal epithelium into the lumen. Within the lumen, the antibodies bind to microbes and toxins and neutralize them by stopping their binding to host cells. This form of humoral immunity is typically called secretory immunity and has advanced to be particularly outstanding in mammals. Studies in mice indicate that IgA responses are made to antigens expressed on only a small fraction of all of the commensal species within the intestine, and these are largely bacteria in the small gut and never the colon. In addition to particularly binding microbes, glycans within the secretory component of IgA (discussed later) can bind to bacteria and cut back their motility, thereby preventing them from reaching the epithelial barrier. It is estimated that a traditional 70-kg grownup secretes about 2 g of IgA per day, which accounts for 60% to 70% of the entire manufacturing of antibodies. Because IgA synthesis happens mainly in mucosal lymphoid tissue and most of the locally produced IgA is effectively transported into the mucosal lumen, this isotype constitutes lower than one-quarter of the antibody in plasma and is a minor component of systemic humoral immunity in contrast with IgG. Several distinctive properties of the gut environment end in selective improvement of IgA-secreting cells that keep in the gastrointestinal tract or, if they enter the circulation, home back to the lamina propria of the intestines. IgA class switching within the gut can occur by T-dependent and T-independent mechanisms. Studies in mice counsel that a lot of the IgA secreted into the lumen is produced by T-independent mechanisms. In each circumstances, the molecules that drive IgA switching embrace a mix of soluble cytokines and membrane proteins on different cell varieties that bind to signaling receptors on B cells (see Chapter 12). The abundance of IgA-producing plasma cells (green) in colon mucosa in contrast with IgG-secreting cells (red) is proven by immunofluorescence staining. Nitric oxide is believed to promote each T-dependent and T-independent IgA class switching. Retinoic acid can also be essential in B cell homing to the gut, as mentioned earlier. However, IgA-secreting plasma cells are widely dispersed within the lamina propria of the gastrointestinal tract, not simply in lymphoid follicles. Secreted IgA is transported via epithelial cells into the intestinal lumen by an Fc receptor called the poly-Ig receptor. Mucosal plasma cells produce abundant J chain, more than plasma cells in nonmucosal tissues, and serum IgA is normally a monomer lacking the J chain. From the lamina propria, the dimeric IgA must be transported throughout the epithelium into the lumen. This function is mediated by the poly-Ig receptor, an integral membrane glycoprotein with five extracellular Ig domains. IgM produced by lamina propria plasma cells can be a polymer (pentamer) related covalently with the J chain, and the poly-Ig receptor additionally transports IgM into intestinal secretions. This receptor is synthesized by mucosal epithelial cells and is expressed on the basal and lateral surfaces of epithelial cells. Dimeric IgA (and pentameric IgM) secreted by plasma cells in the lamina propria bind to the poly-Ig receptor on mucosal epithelial cells by way of a domain of the J chain. The antibody-receptor advanced is endocytosed into the epithelial cell, and unlike different endosomes that sometimes site visitors to lysosomes, poly Igreceptor�containing vesicles are directed to and fuse with the apical (luminal) plasma membrane of the epithelial cell. On the apical cell surface, the poly-Ig receptor is proteolytically cleaved, its transmembrane and cytoplasmic domains are left connected to the epithelial cell, and the extracellular domain of the receptor, carrying the IgA molecule, is released into the intestinal lumen. The cleaved a part of the poly-Ig receptor, referred to as the secretory part, stays related to the dimeric IgA within the lumen. It is believed that the sure secretory part protects IgA (and IgM) from proteolysis by bacterial proteases current in the intestinal lumen, and these antibodies are subsequently able to serve their perform of neutralizing microbes and toxins within the lumen. IgG is current in intestinal secretions at ranges equal to IgM however decrease than IgA. IgA class switching within the gut occurs by both T-dependent and T-independent mechanisms. B, T-independent IgA class switching includes dendritic cell activation of IgM+ B cells, together with B-1 cells. This T cell�independent pathway yields relatively low-affinity IgA antibodies to intestinal micro organism. IgA produced in lymphoid tissues in the mammary gland is secreted into colostrum and mature breast milk by way of poly-Ig receptor�mediated transcytosis and mediates passive mucosal immunity in breast-fed kids. IgA is produced by plasma cells within the lamina propria of mucosal tissue and binds to the poly-Ig receptor at the base of an epithelial cell. The complicated is transported across the epithelial cell, and the sure IgA is released into the lumen by proteolytic cleavage. The process of transport throughout the cell, from the basolateral to the luminal surface in this case, is identified as transcytosis. Moderate quantities of IgG and IgM are additionally secreted into breast milk and contribute to the passive immunity of breast-fed youngsters. Many epidemiologic research have proven that breastfeeding significantly reduces the danger of diarrheal illness and sepsis, particularly in creating countries, and this correlates with the presence of secretory IgA in breast milk particular for enterotoxic species of bacteria including Escherichia coli and Campylobacter. T Cell�Mediated Immunity in the Gastrointestinal Tract T cells play important roles in protection against microbial pathogens within the gastrointestinal system and in regulating responses to food and commensal antigens. Furthermore, T cells contribute to inflammatory diseases within the gastrointestinal tract. In humans, only about 10% of intraepithelial lymphocytes are cells, but this proportion remains to be higher than the percentages of cells amongst T cells in different tissues. This restricted repertoire may have evolved to acknowledge microbes which are generally encountered on the epithelial floor. Dendritic cells and macrophages are plentiful within the gastrointestinal immune system and might take part in stimulating protecting effector T cell responses or inducing regulatory T cell responses that suppress immunity to ingested antigens and commensal organisms.
References
- Pereira C, Murphy K, Jeschke M, et al. Post burn muscle wasting and the effects of treatments. Int J Biochem Cell Biol. 2005;37:1948-1961.
- Koff SA: Mobilization of the urethra in the surgical treatment of hypospadias, J Urol 125(3):394n397, 1981.
- Sasaki M, Yamazaki H, Aoki T, Ota Y, Sekiya R, Kaneko A. Bilateral numb chin syndrome leading to a diagnosis of Burkitt's cell acute lymphocytic leukemia: a case report and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111(3):e11-6.
- VanderLugt J, et al. Efficacy and safety of ibutilide fumarate for the conversion of atrial arrhythmias after cardiac surgery. Circulation 1999;100:369-375.
- Besley GTN, Elleder M. Enzyme activities and phospholipid storage patterns in brain and spleen samples from Niemann- Pick disease variants: a comparison of neuropathic and nonneuropathic forms. J Inherit Metab Dis 1986;9:59.
- Ephgrave KS, Kleinman-Wexler RL, Adar CG: Enteral nutrients prevent stress ulceration and increase intragastric volume, Crit Care Med 18:621, 1990.
- Greenberg DD, Stoker A, Kane S, Cockrell M, Cook JL. Biochemical effects of two different hyaluronic acid products in a co- culture model of osteoarthritis. Osteoarthritis Cartilage 2006; 14(8):814-22.
- Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005;293(17):2126-2130.