

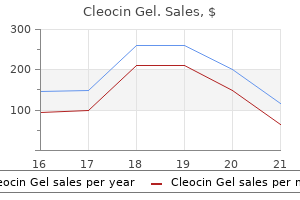
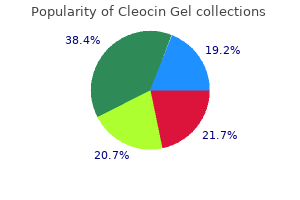
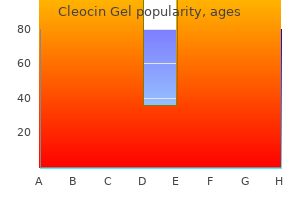
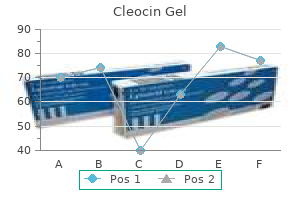
Cleocin Gel
Elizabeth B. Yerkes, MD
- Assistant Professor of Urology, Northwestern University,
- Feinberg School of Medicine
- Attending Urologist,
- Children's Memorial Hospital, Chicago, Illinois
Cleocin Gel dosages: 20 gm
Cleocin Gel packs: 2 creams, 3 creams, 4 creams, 5 creams, 6 creams, 7 creams, 8 creams, 9 creams, 10 creams

Order 20gm cleocin gel overnight delivery
Clinical and radiographic assessment of the younger grownup with symptomatic hip dysplasia skin care in winter buy 20 gm cleocin gel visa. Periacetabular osteotomy without abductor dissection utilizing direct anterior publicity skin care vegetables buy discount cleocin gel 20 gm online. Trochanteric development for premature arrest of the femoral capital development plate skin care summer buy 20 gm cleocin gel otc. Does Dega osteotomy improve acetabular quantity in developmental dysplasia of the hip? Combined pelvic (Dega) and femoral osteotomies in the remedy of paralytic hip dislocation. Chiari pelvic osteotomy for advanced osteoarthritis in patients with hip dysplasia. Shelf operation in congenital dysplasia of the acetabulum and in subluxation and dislocation of the hip. Long term outcomes of Salter and Chiari hip osteotomies in developmental hip dysplasia: a survey of over 10 years follow up with a model new hip evaluation score. Chiari osteotomy in the therapy of the congenital dislocation and subluxation of the hip. Chiari innominate osteotomy in adults: method, indications and contraindications. Medium-term results of the Bernese periacetabular osteotomy within the treatment of symptomatic developmental dysplasia of the hip. Rotational acetabular osteotomy for advanced osteoarthritis secondary to dysplasia of the hip. Intra-articular acetabular labrum: a possible etiological consider certain cases of osteoarthritis of the hip. Chiari pelvic osteotomy for osteoarthritis: the affect of the torn and indifferent acetabular labrum. Computer modeling of surgery and a consideration of the mechanical effects of proximal femoral osteotomies. Intraoperative positioning for arthrodesis of the hip with the double beanbag method. Avascular necrosis following closed discount of congenital dislocation of the hip: evaluation of influencing elements and long-term follow-up. Patterns of ischemic necrosis of the proximal femur in nonoperatively handled congenital hip disease. Lateral tethering of the proximal femoral physis complicating the treatment of congenital hip dysplasia. Risk components of avascular necrosis in the treatment of congenital dislocation of the hip. Growth disturbance of the proximal a half of the femur after remedy for congenital dislocation of the hip. A potential cause of avascular necrosis complicating the therapy of congenital dislocation of the hip. Anatomic and histologic research of factors affecting improvement and evolution of avascular necrosis in congenital hip dislocation. The acute impact of position of immobilization on capital femoral epiphyseal blood move. Avascular necrosis after open reduction for congenital dislocation of the hip: evaluation of causative elements and pure history. Avascular necrosis after non operative remedy of developmental hip dislocation: prognosis in 36 sufferers followed 17Ͳ6 years. Total avascular necrosis of the capital femoral epiphysis in congenital dislocated hips. Vascular epiphyseal adjustments in congenital dislocation of the hip: ends in adults in contrast with results in coxa plana and in congenital dislocation without vascular adjustments. Open discount for congenital hip dislocation: the chance of avascular necrosis with three totally different approaches. A review and assessment of results of therapy with particular reference to frame discount as in contrast with manipulative reduction. An analysis of conservative and operative strategies within the remedy of congenital hip dislocation. The early identification and classification of progress disturbances of the proximal finish of the femur. Acetabular growth in developmental dysplasia of the hip difficult by lateral progress disturbance of the capital femoral epiphysis. Early innominate osteotomy as a treatment for avascular necrosis complicating developmental hip dysplasia. Distal transfer of the higher trochanter revisited: long run comply with up of nine hips. This chapter critiques what is understood concerning the condition, factors out the place controversies exist, and highlights the problems in decision making regarding therapy. The condition was described independently in 1910 by Legg (1), Calv� �2), Perthes (3), and Waldenstrom (4, 5). In the late 19th century, however, Thomas (6), Baker (7), and Wright (8) described sufferers with supposed hip joint infections that resolved without surgical procedure, whose histories have been consistent with Legg-Calv鮐erthes disease. Maydl (9), in 1897, reported this condition and thought it was related to congenital dislocation of the hip (10). In 1909, Arthur Legg offered a paper on 5 youngsters who had been limping after harm. He known as this condition an "obscure affectation of the hip" and postulated that stress secondary to damage caused flattening of the femoral head (1). In that same 12 months, Calv顲eported 10 circumstances of a noninflammatory self-limiting condition that healed with flattening of the weight-bearing floor. He postulated that the trigger of this situation was an abnormal or delayed osteogenesis. He reported coxa vara and elevated femoral head measurement in these patients; on bodily examination, all of the sufferers had decreased abduction (2). Perthes concurrently reported six instances of what he termed "arthritis deformans juveniles. In his description of the condition, Waldenstrom postulated that the disease was a form of tuberculosis (4, 5). Perthes was the first investigator to describe the pathologic and histologic options of the disorder (11). Examination of a portion of the excised head revealed numerous cartilage islands throughout and "strings" connecting the cartilage of the joint and the physeal plate. Perthes noted that the marrow areas had been widened, with fatty infiltration; he noticed no proof of irritation.
Periploca of the Woods (Gymnema). Cleocin Gel.
- Diabetes, metabolic syndrome, weight loss, stimulating digestion, malaria, cough, snake bites, softening the stool (laxative), and increasing urine excretion (diuretic).
- Are there safety concerns?
- How does Gymnema work?
- Dosing considerations for Gymnema.
- Are there any interactions with medications?
- What is Gymnema?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96816
Buy cleocin gel 20gm on line
Dashed line signifies the position of the indirect osteotomy between the anterior and center facets of the calcaneus acne 101e discount 20 gm cleocin gel with amex. B acne 11 year old boy buy cleocin gel 20 gm with amex, C: Insertion of the trapezoid-shaped tricortical iliac crest bone graft corrects all parts of the valgus deformity of the hindfoot skin care over 50 purchase cleocin gel 20 gm without prescription. D: A plantar-based closing-wedge osteotomy of the medial cuneiform corrects the supination deformity of the forefoot. Lengthening of the gastrocnemius or the Achilles tendon is almost always needed. If desired, the pin could be removed within the workplace after 6 weeks and the forged modified. Although this was merely a description of the anatomic shapes of the bones, they used their findings to condemn the calcaneal lengthening osteotomy. Despite presenting no medical knowledge, they argued that the osteotomy is intra-articular and would doubtless trigger degenerative modifications within the subtalar joint. Evans (236) could, actually, have created a true intra-articular osteotomy typically. The very fact that there are so many anatomic variations in the measurement, shape, and even existence of the anterior aspect speaks to the attainable insignificance of that construction (358). It is plantar-lateral and seems to act merely as an attachment point for the spring ligament (358). Additionally, the most important displacement of the calcaneal fragments happens laterally, away from the aspects. Other authors have subsequently confirmed the efficacy of the calcaneal lengthening osteotomy for relieving pain and correcting deformity in painful flatfeet (359ͳ67). In abstract, if the requisite indication for the calcaneal lengthening osteotomy is intractable pain in a flatfoot with a short Achilles tendon, the relative risk of a theoretically intraarticular osteotomy compared with the reported glorious clinical results of the procedure is obviated. Like Kohler illness, Freiberg infraction is taken into account to be an osteochondrosis, an idiopathic situation characterised by disorderliness of endochondral ossification. However, unlike Kohler illness, it has been classified by Siffert (369) as a main articular osteochondrosis which will or might not progress to disruption of the subjacent bony epiphysis. These histologic adjustments happen in constitutionally and biologically prone metatarsal heads for unknown causes. Proposed theories embrace trauma, repetitive stress, vascular anomalies, and high-heel shoe wear (370, 371). In 1914, Freiberg (368) described a painful condition of the second metatarsal head that was characterised by flattening of the articular surface of bone with areas of each lucency and sclerosis. Postulating a traumatic origin, he labeled it an "infraction" rather than an "infarction," which might imply an ischemic origin. There is softtissue swelling, tenderness, and restriction of motion of the involved metatarsophalangeal joint. The radiographic findings of Freiberg infraction, just like the bodily findings, are varied and have a tendency to correlate with the pathologic stage of the illness, however not essentially with the bodily complaints. The incidence of this condition is unknown, however it happens mostly in adolescent women and is, surprisingly, the one "osteochondrosis" with a predilection for the feminine sex. The second metatarsal is mostly affected, followed by the third, whereas the primary, fourth, and fifth are hardly ever concerned. The intra-articular and periarticular gentle tissues are thickened and edematous through the first stage. In the second stage, the cells of the epiphysis that receive vitamin by diffusion from the joint fluid are disadvantaged on account of the edematous strain from chronic synovitis. Blood vessels throughout the epiphysis are incompetent secondary to thrombosis or microfractures of the trabeculae. The epiphyseal contour becomes deformed because of this disordered osteogenesis and chondrogenesis. Repair takes place through the third stage with gradual replacement of the necrotic bone. Alternatively, the necrotic bone segment(s) might separate as an intra-articular unfastened body leaving a defect in the articular floor. It is far more frequent in girls than boys, with ladies accounting for over 80% of operative cases (378). Studies and case reviews indicate that juvenile hallux valgus could additionally be associated with both an X-linked dominant, autosomal dominant with very variable penetrance, or polygenic transmission (378, 381). Most adolescents with hallux valgus are asymptomatic and have realized to choose their shoe wear in order to avoid pressure and pain on the medial aspect of the first metatarsal head. Others report ache solely when sporting sure style sneakers that match poorly and are biomechanically inferior. The pain is positioned within the superficial medial delicate tissues because of stress from the shoe on the bony prominence of the first metatarsal head. Look for other causes of ache surrounding the metatarsalΰhalangeal joint similar to arthritis, infection, or lesions of the local soft tissues or bone. There can also be pain associated with the overlapping of the second toe on the distal finish of the hallux. The foot ought to be assessed in weight bearing to decide the alignment of the midfoot and hindfoot, looking in particular for related flatfoot deformity. The disease generally progresses by way of the three phases described in the preceding text, with reconstitution of a passable articular floor and reduction of pain. The long-term results depend upon the severity of the harm to the articular surface and whether loose our bodies outcome. Nonoperative remedy is indicated to relieve signs and to allow therapeutic, as will happen in lots of cases. Modalities embrace restriction of actions, avoidance of weight bearing, forged immobilization, metatarsal bars and other shoe inserts to relieve strain beneath the metatarsal head, and modification of shoe put on. Avoiding high-heeled shoes that place more stress on the metatarsal heads is suggested. Surgical options include joint debridement and elimination of free bodies (368, 372, 375), elevation of a collapsed articular surface with bone grafting (373), excision of a metatarsal head and shortening of a metatarsal (376), and metatarsal dorsiflexion osteotomy (371, 372, 375). Debridement of periarticular osteophytes or outstanding bone impinging on metatarsalΰhalangeal joint movement is a procedure that normally gives satisfactory symptomatic reduction (368, 372, 377) if required. The addition of a distal metatarsal dorsiflexion osteotomy has been reported to relieve signs and to restore joint movement (371, 372, 377). Attention to the major points of the process is essential to have the ability to avoid iatrogenic disruption of the vascularity of the metatarsal head and to avoid the creation of switch lesions to adjacent metatarsal heads (371). Standing anteroposterior and lateral radiographs of the foot are necessary to consider juvenile hallux valgus. Assessment of overall foot alignment, together with the midfoot and hindfoot, is essential. Unfortunately, identification of the location of the articular cartilage on the metatarsal head is difficult on radiographs of the feet of youngsters and many adolescents. Juvenile hallux valgus is outlined as >14 levels of lateral deviation of the hallux on the first metatarsal that has its onset in preteenage or teenage years when the expansion plates of the first metatarsal and proximal phalanx are still open.
Generic 20gm cleocin gel otc
Current options for administration embrace immobilization without making an attempt discount acne face mask proven cleocin gel 20gm, or discount beneath sedation or anesthesia with assessment of postreduction stability skin care 30 years old buy cleocin gel 20 gm otc, and percutaneous fixation if unstable skin care routine for oily skin generic cleocin gel 20gm amex. Some practitioners also consider that accidents to the dominant arm of a throwing athlete also wants to be handled with discount and fixation. If unstable, the fracture was handled with percutaneous pin fixation and immobilization. The indications for operative administration of adolescent proximal Closed Reduction Method. In most fractures, the distal fragment will be displaced anteriorly via the thinner periosteum, and the proximal fragment will be abducted and externally rotated by its muscular attachments. After enough analgesia and/or anesthesia, longitudinal traction is utilized to the injured extremity, and the distal humeral fragment is flexed, kidnapped, and externally rotated. Posteriorly directed strain during flexion on the distal fragment will push it again inside the soft-tissue envelope, after which abduction and exterior rotation will cut back the fragment. Fluoroscopy is helpful to assess the position of the fracture fragments throughout discount. If the fracture redisplaces to an unacceptable diploma with the arm on the aspect, then repeat discount and percutaneous pin fixation is warranted. For minor quantities of residual varus, an abduction pillow on the facet with the sling and swathe could also be used. For unstable fractures and irreducible fractures, the affected person ought to be taken to the operating room for basic anesthesia. The affected person is positioned supine on the fringe of a very radiolucent desk to facilitate fluoroscopy. The arm and shoulder are sterilely prepared and draped, and repeat closed discount is attempted. Because of the danger of migration with use of easy pins, some favor pins with threaded suggestions, and it is suggested to place a big bend in the end of the pins left outdoors the skin. The axillary nerve is in danger, and runs from posterior to anterior around the proximal humerus in a zone 5 to 7 cm distal to the tip of the acromion. Pins ought to thus begin distal to this, and are placed from the lateral proximal humeral metaphysis and directed up and into the humeral epiphysis. The first pin starts anterolaterally, and then a second pin is positioned anterior or posterior to the primary, with an attempt to get some divergence or spread of the pins in the epiphysis to enhance stability. HΊ: the affected person has recovered full range of motion, but has a 1-cm arm-length discrepancy. The proximal fragment is kidnapped and externally rotated due to the rotator cuff attachments. The shaft is displaced proximally by the pull of the deltoid muscle and is usually adducted by the action of the pectoralis muscle. The arm is externally rotated and kidnapped with longitudinal traction to achieve this position. D There usually is a posteromedial Thurston-Holland fragment, and if large enough one pin can keep below the physis and have interaction this fragment. If screws crossing the physis are used, screw elimination may be indicated if substantial development potential stays. The long head of the biceps tendon or periosteum could additionally be interposed obstructing an accurate discount. After fixation, the arm is immobilized with a sling and swathe for three to 4 weeks, at which era radiographs are taken to assess therapeutic, and the pins are eliminated. Other humeral shaft fractures in kids younger than 3 years are sometimes the results of nonaccidental harm (30). In fractures with radial nerve palsy, the prognosis for neurologic restoration is excellent. Nerve injury with closed fractures of the humerus ought to be noticed for 3 to 5 months earlier than contemplating intervention. Infants could also be handled with mild positioning and swaddling, with a small coaptation splint, or the arm may be splinted in extension, using a small splint or a tongue blade and tape. A, B: Radiographs of severely displaced fracture that was unstable after reduction and stabilized with distal to proximal pins, with pins bent exterior pores and skin. B deformity and shortening can be anticipated in infants and younger kids, with up to 65 degrees of angulation remodeling documented in infants (31). Older youngsters could additionally be treated with a coaptation splint and a sling to preserve alignment of the arm. Occasionally, an abduction splint or pillow could additionally be used to management varus alignment. In older youngsters and adolescents, complete displacement and a pair of cm of shortening are acceptable. Up to 20 levels of angulation is appropriate within the middle third and 15 degrees in the distal third of the humeral shaft (32). Greater degrees of deformity are often unacceptable cosmetically, though they could transform without inflicting functional issues. Indications for surgical procedure embody open fractures, a number of injuries, and ipsilateral forearm fractures in adolescents. Open or comminuted fractures could be stabilized with an exterior fixator till union is complete or till fracture stability and wound therapeutic permit changing to splint immobilization. Rare open proximal humeral physeal fracture handled with open reduction and fixation with two screws, three weeks after fixation. Retrograde insertion is appropriate for fractures of the diaphyseal and proximal humerus. Antegrade insertion is completed by passing a single rod by way of a portal in the area of the higher tuberosity. A larger deltoid-splitting incision can be utilized to create a portal giant sufficient for two versatile rods to be inserted if wanted for extra stability. Usually the discount is sufficiently stable to permit use of a sling or a shoulder immobilizer; however, a coaptation splint or above-elbow cast could also be applied. Healing is usually adequate within 3 to 4 weeks to provoke range-of-motion workout routines. Only full vary of movement, complete absence of swelling, and normal radiographs warrant the prognosis of elbow sprain or contusion. A clinical rule of thumb is that if a child can fully extend the elbow with minimal discomfort, an elbow fracture is unlikely. Small fractures that seem to be avulsions must be accurately identified, because they could indicate a serious injury similar to an associated elbow dislocation. Precisely defining the fracture patterns is a challenge in younger youngsters because of the large cartilage composition concerning the elbow.
Generic cleocin gel 20 gm free shipping
Prophylactic pinning must be carried out for kids with underlying endocrine illness because of their high fee of contralateral slip acne under beard discount 20 gm cleocin gel overnight delivery. Previous pelvic radiation skin care at 30 cleocin gel 20 gm with amex, which included the contralateral hip within the subject skin care myths purchase 20gm cleocin gel with mastercard, is one other indication for prophylactic pinning. In children with renal illness, medical management somewhat than prophylactic pinning is beneficial. At the time of re-presentation, anteroposterior (C) and frog lateral (D) radiographs show marked slip of the previously regular proper hip. Femoral neck osteoplasty includes elimination of the outstanding anterosuperior femoral neck and could additionally be performed alone or in combination with other procedures, such as proximal femoral osteotomies (124, 342, 343). Symptoms that may counsel the potential benefit of osteoplasty embrace ache on sitting attributable to the impingement with hip flexion. If performed in isolation, osteoplasty leaves unchanged the irregular relation between the femoral head, neck, and shaft, with relative retroversion, extension, and varus. Previous authors have noted that osteoplasty might further improve hip range of movement following intertrochanteric osteotomies (124, 342, 343). Hall (275) noted that complications had been the one factor that appeared to result in an early poor outcome. At a imply follow-up of forty one years, Carney and Weinstein (167) reported Iowa hip scores of a minimum of 80 in 26 of 31 hips (84%). Hagglund (269) famous that no hip with a gentle or average slip treated with in situ pinning developed arthritis earlier than 50 years of age. Recent authors have sought to forestall late arthritis by restoring extra normal proximal femoral anatomy by performing proximal femoral redirectional osteotomies (89, 292). In these two sequence, the general breakdown of slips was 76% chronic, 21% acute-on-chronic, and 3% acute. The mixture of anti-inflammatory medicines, physical remedy, and guarded weight bearing could additionally be helpful in sustaining the vary of movement and stopping progressive femoral head collapse. When femoral head collapse occurs within the area of beforehand placed screws, the screws should often be backed out or removed in order to forestall joint penetration and chondrolysis. With progressive collapse and joint degeneration, salvage procedures are sometimes needed. Impact activities such as operating, leaping, and ball sports must be prevented, whereas swimming and bicycling may be undertaken to preserve cardiovascular health, strength, and vary of movement. Anti-inflammatory medicines and ambulatory aids may be helpful as nicely, though these are often rejected by otherwise wholesome adolescents and younger adults. Normal cartilage thickness of the pediatric hip has been reported to lower from a imply of 6 mm in children aged 1 to 7 years, to 5 mm in those aged eight to 12 years, and to four mm in those aged 13 to 17 years (355). Unlike many different hip maladies, chondrolysis causes the hip to be held in abduction and finally ends in a exhausting and fast abduction contracture. Chondrolysis is extra common in the female population than in the male population (243, 245, 359). Previously, chondrolysis was believed to be extra common in black youngsters (76, a hundred and eighty, 212, 243, 356, 360), although more recent research have refuted this assertion (202, 216, 243, 360, 361). One collection reported a higher incidence of chondrolysis in these of Hawaiian descent (357). Ten months later, the affected person introduced to the office with a 1-month historical past of left hip ache. However, 2 months postoperatively the affected person began to have increased hip pain, difficulty walking, and decreased hip range of motion. Chondrolysis is seen following all types of remedy and has also been reported to be present at the time of preliminary presentation in some patients (243, 245). Maurer and Larsen (357) suggested that chondrolysis was extra widespread with extreme slips and with spica casting, open discount, or prolonged casting. Chondrolysis within the unaffected hip has been reported following immobilization (32, 183). Rates of chondrolysis are commonly reported as 3% to 18% following subcapital osteotomy (256, 296, 297, 301, 302, 307), 2% to 10% following base-of-neck osteotomy (264, 308), and 2% to 25% following intertrochanteric osteotomy (124, 243, 289, 310, 322, 324, 327). Reported rates of chondrolysis following in situ pinning and bone peg epiphysiodesis are most commonly <5% (2, 24, 30, one hundred twenty five, 181, 186ͱ88, 196, 199, 202, 204, 208, 212, 216, 220, 228, 243). In addition to narrowing of the joint house, radiographs may reveal untimely closure of the apophysis of the larger and lesser trochanters (243, 362). Bone scan has been noted to demonstrate decreased exercise in the apophysis of the greater trochanter in 47% of hips affected with chondrolysis, a discovering that may precede radiographic changes (363). In circumstances with an unusual presentation, workup for a septic hip together with joint aspiration could also be indicated. Chondrolysis varies from a comparatively minor, self-limited condition from which full restoration may occur to the rapid destruction of a joint necessitating salvage therapy in teenagers (245, 358, 364). Despite many years of experience in treating youngsters with chondrolysis, the explanations for such disparate prognoses stay unclear. Treatment of chondrolysis is usually conservative, with a mixture of protected weight bearing, physical therapy (for vary of motion and tried strengthening of the hip musculature), and oral anti-inflammatory drugs. Distraction of the hip joint with exterior fixation has been reported to be of worth in selected circumstances (365). Failure of such conservative measures might require surgical intervention similar to arthrodesis or arthroplasty. Early recognition and treatment are indicated, however the prognosis following this complication is guarded. In sufferers unresponsive to conservative measures, salvage procedures could additionally be needed. The extent of hip illness in both hips is important in making the decision regarding hip arthrodesis versus arthroplasty. Currently, many youngsters and their households are reluctant to settle for the bodily limitations associated with hip arthrodesis, despite the lower than stellar outcomes of hip arthroplasty in younger patients. An articulation between metallic and ultrahigh-molecularweight polyethylene has been the gold commonplace since the earliest complete joint replacements. The long-term leads to young patients have been inferior to these in older sufferers, with much of the loosening attributable to the era of particulate debris and component loosening (171, 368ͳ71). New bearing surfaces corresponding to those together with highly crosslinked polymers, metal-on-metal, and ceramics have given hope to a model new era of surgeons and sufferers about the potential for hip arthroplasty in the young and energetic inhabitants. Many procedures have been described for hip fusion including intra-articular and extra-articular fusion using quite lots of fixation devices together with screws, plates, and exterior fixation (372ͳ77). The commonest hip fusion technique in children currently is an intra-articular fusion with subtrochanteric osteotomy, which has been reported by a number of authors since it was first reported by Farkas in 1939 (374, 378ͳ80). This method is felt to promote fusion because contact between the femoral head and acetabulum may be maximized and the lengthy lever arm of the leg is averted by performing the subtrochanteric osteotomy. The advantages of hip fusion embody the sturdiness of the fusion and the power to return to full activity, together with guide labor. Long-term ends in research with mean followup exceeding 35 years have been quite satisfying, although reported findings include back pain in 57% to 61%, ipsilateral knee pain in 45% to 57%, and contralateral hip ache in 17% to 27% (373, 377).
Effective 20 gm cleocin gel
Each 12 months zone stop acne - buy 20gm cleocin gel mastercard, above the age of 17 skin care 20s purchase cleocin gel 20 gm visa, the chance for stress fractures was noted to have been reduced by 28% (367) acne face wash discount cleocin gel 20 gm visa. A retrospective review was carried out on 154 navy patients aged 17 to 29, and of the 143 stress fractures recognized 99% have been located at the tibia (368). Many components have been correlated with stress accidents in pediatric athletes together with an excessive rate of train progression, anatomic malalignment, a historical past of stress injuries, adjustments in energy and adaptability associated with progress, and elevated body mass index (366). A wellunderstood risk for stress fractures is a rapid improve in training depth which can be generally found in younger athletes implementing new training protocols or starting team preseason training regimens. The female athlete triad of menstrual irregularity, osteopenia, and disordered eating should alert the treating physician to the potential for an elevated risk for stress injuries. A distinction was famous in cumulative stress fractures with an incidence of 4% in girls with a daily menstrual historical past versus 15% in girls with irregular or absent menses (369). A prospective, multicenter cohort research was carried out to examine threat factors, and among 146 collegiate athletes these more prone to develop medial tibial stress Stress Fractures. Stress fractures are becoming extra widespread in kids due to an elevated degree of participation in organized athletics, earlier sports specialization, yearround sports activities, and participation in multiple teams during the same season. Stress fractures come up from repeated submaximal stresses applied to normal bone or regular stresses applied to irregular bone and may current as a spectrum spanning from a light microfracture to an entire fracture. In a study of adolescent athletes with open physes, patients have been primarily handled with discount in weight bearing; nonetheless, 7 of 21 sufferers reported unsatisfactory outcomes and four patients with tibial stress fractures had persistent signs and have been modified from decreased weight bearing to plaster solid immobilization. Risk elements for tibial stress fractures embrace hip exterior rotation, knee malalignment, smaller tibial width, a poor level of conditioning, exhausting terrain, in addition to nutritional elements. The main concern in analysis is differentiating a stress fracture from a malignant bone tumor, especially with some periosteal new bone formation. The physician should also rule out other situations similar to benign tumors together with osteoid osteoma, infection, inflammatory arthritis, or soft-tissue harm. Shin splints are discomfort in the leg from musculotendinous inflammation on account of repetitive impact exercises or the utilization of foot flexors in sports activities corresponding to working. In patients with proximal discomfort, the examiner should verify for referred ache from the patellofemoral area as sufferers with the horrible triad of femoral anteversion, genu valgum, and pes planus. This terrible triad of malalignment points is a predisposing factor within the growth of overuse accidents of the patellofemoral area and the decrease legs. When assessing a younger athlete in whom an overuse damage is suspected a cautious and detailed history is important in differentiating stress fractures from different circumstances. Night pain is unusual in stress fractures but is frequent is osteoid osteoma or malignant bone tumors such as osteogenic and Ewing sarcoma. The bodily examination ought to include an analysis of the entire kinetic chain together with alignment, gait, limb length, muscle energy, and flexibility which can reveal tightness, acceptable flexibility, or pathologic laxity. Stress fractures are noted to occur extra generally in athletes with foot abnormalities corresponding to pes cavus and pes planus (366, 371ͳ73). Technetium scans are useful to affirm the diagnosis of a stress fracture, and adjustments could be famous utilizing this system as early as 12 to 15 days following the onset of harm and signs. It can at instances be challenging utilizing bone scintigraphy to distinguish the difference between a stress fracture of the bone and shin splints from musculotendinous irritation. The activity modification contains schooling and instruction for the young athlete to partake in train that does impart forces on the injured area. This at times consists of eliminating the game that the athlete participates in altogether. Bracing for lower extremity stress fractures might include boot or forged immobilization or off-the-counter orthotics for 4 to 6 weeks to enable adequate bone deposition to occur. Continued rehabilitation and prevention consists of advancement to strengthening, flexibility workout routines and training, in addition to instruction concerning already addressed factors in the workup including nutritional influences, graduated coaching regimen will increase, and an consciousness of coaching surfaces. There are some anatomical areas that are susceptible to prolonged symptoms or in some circumstances nonunion together with the femoral neck, tibial diaphysis, medial malleolus, and tarsal navicular (366). Femoral shaft stress fractures are at low threat of nonunion or displacement and could be managed with activity modification. Surgical treatment is due to this fact really helpful and is most commonly carried out with cannulated compression screws. For tibial stress fractures, the posterior medial compression facet stress fracture is the most typical. This is a low-risk stress fracture and most heal with four to 6 weeks of pneumatic boot immobilization. The tibial anterior tension facet fracture is much less common; nevertheless on this hypovascular region, callus is generally not fashioned and patients are at risk for delayed union or nonunion (378). In the case of delayed union, a patellar tendon-bearing cast or commercial orthosis should be employed for 4 to 6 months earlier than surgery is taken into account. If nonunion exists within the skeletally mature adolescent, options to treat the nonunion include the use of an intramedullary nail with or with out bone grafting and fibular osteotomy (379). In the skeletally immature particular person with a diaphyseal tibial stress fracture that fails to heal after 6 months of nonoperative therapy, operative remedy is indicated. Excision of the fibrous nonunion and autogenous bone grafting from the iliac crest with possible fibular osteotomy has been employed successfully on this rare scenario (379). For medial malleolus stress fractures, the fracture line tends to traverse in an oblique method from the intersection of the medial malleolus and the tibial plafond. Nonoperative administration together with restricted weight bearing as nicely as casting or bracing has the next failure rate than different low-risk fractures. Operative intervention due to this fact may be performed to facilitate early healing and recovery. In the case of nonunion of tarsal navicular stress fractures, recommended therapy contains excision of the nonunion web site and autogenous bone grafting. In the case of 5th metatarsal fracture nonunion, beneficial remedy includes intramedullary screw fixation with or without bone grafting. While the greatest concern for a younger athlete is the timeliness of return to sports, the treating doctor must assess multiple variables. Return to play ought to be guided by elements indicative of therapeutic and injury prevention including the cessation of pain, radiographic proof of a healed fracture, elimination of inciting causes and instruction concerning coaching methods, and a graduated train program. Sever calcaneal apophysitis is a self-limited inflammatory situation of the os calcis in growing children. The typical child with Sever illness is from 9 to 14 years of age and concerned in operating sports activities (380). The condition is bilateral generally and presents as diffuse ache and tenderness over the prominence of the heel quite than solely on the plantar facet as is seen in plantar fasciitis (381). With relaxation, exercise modification, and passage of time, the situation always resolves (380, 382, 383). Cast immobilization could rarely be necessary for the affected person with severe, incapacitating signs (383). Repetitive stress within the upper extremity might result in a particular stress reaction in the physis.
Buy generic cleocin gel 20 gm
This is just like 302 skincare 20gm cleocin gel fast delivery performing a Marquardt procedure and has the potential to considerably scale back problems of overgrowth acne vulgaris cause generic 20 gm cleocin gel overnight delivery. Children with neurofibromatosis acne 10 gel buy 20 gm cleocin gel amex, KlippelTrenaunay-Weber syndrome, and malignant tumors not suitable for limb salvage are also on this class. In many instances, the necessity is obvious, and the kid and fogeys have accepted their choice after cautious consideration. In all circumstances, the more preparation by the medical professionals and alternatives for the dad and mom and affected person to discuss and see other patients, the better. It needs to be emphasised that the challenge to be overcome with remedy is to reside, and that the surgery is important for that. The options revolve around the useful and cosmetic aspects of the completely different procedures. However, in the older child, especially when the amputation is brought on by trauma, there may be large psychological benefits from putting the kid instantly in a postoperative prosthesis. When dealing with the adult inhabitants, overall biomechanical forces ensuing from prosthetic alignment can do comparatively little injury to skeletal integrity. Rigid time schedules are discouraged, and developmental ranges should be used only as a tough guideline to assist the practitioner. Fitting the child with limb deficiency leads to distinctive issues not usually seen in the grownup population. Knee disarticulations can result in lengthy residual limbs with knee centers decrease than on the sound aspect. Location of bony landmarks is obscured by fatty tissue, and casting is troublesome and nonexact. The various levels involved prior to becoming a prosthesis are typically normal inside the profession. Upon referral to a clinic, the kid is assessed by the staff, and a remedy protocol is established. The role of the prosthetist is to be positive that the highest stage of practical need of the affected person is met through prosthetic intervention, or via no intervention at all if indicated. The skilled prosthetist can assess anatomic and functional deficiencies and recommend socket design and element choice. In recent years, there was an incredible enhance in the prosthetic improvements and elements available for the pediatric amputee. Knowledge of these elements and their appropriate use will typically be the accountability of a prosthetist with particular curiosity and experience with kids. In addition, she or he must possess the medical expertise, medical data, and communication skills to timely direct the circulate of data to the opposite staff members and parents, so that realistic expectations may be identified and achieved. Routine maintenance of the prosthesis is extraordinarily important so that in depth repairs shall be minimized and the need for a brand new prosthesis recognized. It is simply after a well-fitting and comfortable socket skin interface is achieved that the additional elements may be added and expected to function as designed. Casting normally involves the putting of a casting sock on the residual limb, marking all landmarks and wrapping circumferentially with plaster or artificial bandage. It is then filled with molding plaster and stripped, forming the optimistic solid ready for modification. This constructive cast is then modified to distribute forces and relieve pressure in the socket for correct hydrostatic control of the residual limb. Common fitting problems could be flagged and corrected earlier than the ultimate socket design. The info is relayed to a pc, with which modifications can be made to the scanned form to allow for increased or decreased weight-bearing areas. The finished design is transferred to a computerized milling machine to kind a positive mannequin. During dynamic alignment in the crawling toddler, the prosthetist initially focuses on making a prosthesis that may Fitting Techniques. The technique will vary, on the idea of prosthetist expertise, group philosophy, integration of ever-changing know-how, and severity of the deficiency. Physiologically, the kid is in a continuing state of development and the prosthetic device have to be designed each to allow weight bearing and to allow for the greatest amount of development with out compromising match and function. Most congenital decrease extremity amputees are capable of bear some weight on the distal finish of the residual limb, permitting the prosthetist to achieve a slightly much less intimate match of the prosthetic socket than might be the case for the acquired grownup amputee. The elevated activity ranges of the child amputee place tremendous expectations on the prosthetic devices and the elements. All of these factors are constant challenges to the prosthetic prescription and emphasize the necessity for a fluid method to fitting. Sutherland concluded that mature gait patterns were established by 3 years of age (219), whereas others place the timeframe closer to 6 years of age. Early toddler gait patterns are, actually, the processes of suppression of primitive reflexes and the acquisition of postural responses (220). Dynamic alignment is the manipulation of relative position of the socket to the foot and knee while the prosthesis is shifting by way of the various phases of gait. Through the usage of alignment mechanisms in the components, the prosthetist is prepared to shift, tilt, and rotate the knee and foot in relation to the socket. Once impartial gait is established within the infant, refinement to gait can be achieved through additional prosthetic alignment. Children with amputations at this level can achieve outstanding gains when fitting begins whereas the kid is pulling to stand and when therapeutic intervention and parental coaching are incorporated. It is really helpful that the knee be locked, initially, in order that hip control can first be realized. The underlying principle is to adduct the femur whereas locking the ischial tuberosity inside the socket, thereby providing a extra anatomically appropriate alignment during all phases of gait (222). The controversy over these designs has been more and more dispelled, with further scientific experience. There are numerous suspension mechanisms which could be utilized for the safe attachment of the socket to the residual limb. These gadgets may present auxiliary suspension which is hooked up to the socket to suspend or enhance suspension. The Silesian belt attaches to the anterior/medial facet and the lateral facet of the transfemoral socket and lies across the pelvis at the waist. The accommodation for differences in tissue compressibility, pressure tolerance, underlying bony structures, and vascular integrity are elements taken into account previous to socket design. Dynamic forces exerted by way of ground response forces and ensuing moments, including torque and shear forces, increase the vulnerability of the skinγocket interface. Amputees on the hip disarticulation degree require intensive prosthetic intervention. The socket encompasses the amputated pelvic remnant and encloses the contralateral side for suspension. The conventional socket design rises proximally to the waist and suits equally to a Boston spinal orthosis. The diagonal socket is a modified version of the standard design, and it affords a more comfortable match and increased flexibility.
Syndromes
- Opening of the edges of your intestines that are sewn together (anastomotic leak), which may cause life-threatening problems
- Have you recently had a vaginal or uterine infection?
- Myelodysplasia (MDS)
- Stiff neck
- Drink plenty of water (8 to 10 cups) every day.
- Identify risks for heart disease
- 1 tbsp mayo-type salad dressing
- Diarrhea and other infections that last a long time, such as parasites
Cleocin gel 20gm for sale
The prosthetic knee unit could be additional subdivided into single axis and polycentric types acne 5 buy cleocin gel 20gm low cost. The maturation of gait from infant to adult carries with it the need for sound apply in deciding on the suitable knee acne yellow pus best 20 gm cleocin gel, on the idea of amputation level acne wash cleocin gel 20gm free shipping, practical stage, and body dimension. In common, the single-axis internal knee without any control unit is the primary knee to be used on the kid, because of its gentle weight, short lever arm, and ease. In the single-axis knee joint, the decrease shank rotates around a single point in relation to the socket. A polycentric knee was introduced in 1998 for the toddler and toddler, and it might be used if area permits. Internal polycentric knees move round a middle of rotation that varies with the flexion angle of the lower shank (213). The inherent stability throughout stance, the fluid knee-flexion movement, and the mechanical design to give extra floor clearance throughout flexion improve patient and practitioner confidence in the unit (225). Variations within the supplies, design, and alignment of the foot can have profound effects on the efficiency of the prosthesis. Four-bar linkage is an internal polycentric knee that gives many advantages to the patient, including increased stability and higher ground clearance throughout swing section. As indicated on this illustration, the purpose of rotation varies with the diploma of flexion. With the knee flexed, the leg folds underneath the thigh segment and subsequently may be very useful for longer residual limbs. Traditionally, an articulating knee would be introduced in a congenital amputee at roughly three to 4 years of age. This age was determined, partly, by the constraints in the size and function of the parts. A current report demonstrated the benefits of early fitting with articulated knees in kids as young as 17 months. All children discovered to walk with an articulated knee, regardless of their age variations (157). Most elements carry particular weight tips, and many children attain these ranges well before adulthood. For example, an adult hydraulic polycentric knee is routinely used on 8-year-old boys whose weight has surpassed one hundred lb. It is usually considered when amputees require maximum late-stance stability due to weak knee extensors, knee-flexion contractures, or poor midto late-stance balance (227). By altering the hardness of the bumper, the prosthetist is prepared to successfully change the properties of the foot. This foot is greatest suited for the transfemoral amputee, in whom full-foot contact with the bottom is necessary to increase stability. The multiaxis foot allows passive dorsi- and plantar flexion, inversion, and eversion. The multiaxis foot was once thought best suited for the amputee who because of uneven terrain or a method of life that features golfing or varied sports requires flexibility and a few rotational management: It has now discovered its way into the pediatric population. This class of foot has gained extensive acceptance throughout the pediatric enviornment, partially because of its capability to take up forces at the ankle and cut back transmission of those forces to the socket. The dynamic-response foot has found its means into competitive-level sports activities in addition to day-to-day activities. It is necessary to use parts that will maximize performance and on the same time be applicable for the patient (228). B: the Little Feet kind design incorporates unique power dynamics with flexible toes all in sizes beginning at 10-cm length. The length of the keel controls the toe lever arm and thus the hyperextension second at the knee, and the compression of the elastomer heel absorbs and deflects the forces at heel strike. C: the dynamic multiaxial TruPer foot allows rotation, inversion and eversion, flexion, and extension movements. It is used for the older, stronger, and bodily lively youngster who has the physical capability to use such a foot. The involvement in aggressive sports activities is usually a great benchmark to provoke fitting adolescents with the highestperformance dynamic-response ft. The identical is true of the transtibial amputee, who lacks the muscle power to control the foot, usually resulting in premature muscle fatigue. In the choice of a quantity of elements, the prosthetist should marry the characteristics of all components, in order that most profit could be obtainable to the amputee. The most essential consideration within the becoming of the partial-foot amputee is to ensure that adequate load-bearing is designed into the prosthesis of choice. As a common rule, the extra proximal the extent of amputation, the higher the prosthesis should match over the ankle complex and the more proximally it must match on the tibia and fibula. Tissue condition, operate of the remaining foot advanced, and exercise of the kid all play a job in figuring out the prescription and design of the prosthesis. Complete or partial absence of the toes usually requires little greater than a shoe filler. A carbon fiber insert to better management forces from heel to toe-off could also be included in the shoe filler. In the case of the very younger baby, no intervention may be required until a necessity has been demonstrated, for instance, the lack to keep the shoe on, particularly when the kid becomes extra active in sports. This incorporates a cosmetic foot shell, silicone-laminated socket with modified foot sole, and a posterior zipper for ease of donning and doffing. The socket trim line is proximal to the malleoli and is fitted intimately to guarantee adequate management. The design of a partialfoot prosthesis can also embrace a detachable insert, to accommodate the necessity for corrective alignment of the residual foot. Overall, this type of prosthesis is perfectly suited to the child amputee and resists untimely wear and tear. If needed, a partial-foot prosthesis ought to be prescribed once the child is pulling to furnishings, in order that foot control will start at an early age. It must be noted that a low-profile insert (distal to the malleoli), used at the facet of a hightop boot, will supply enough operate and cosmesis till a decrease reduce shoe is requested by the parent. The prosthesis must encompass the ankle joint, and it usually rises proximally to the patellar tendon in an effort to cut back forces on the tibial crestγocket interface. Selection of prosthetic toes is compromised because of the shortage of area distally, and commercially obtainable carbon foot plates require permanent attachment with vulcanizing rubber cement. This negates any modifications brought on by development, and realignment to compensate for gait modifications is just about inconceivable. The choices left open to the prosthetist are numerous and, at occasions, controversial. Where some clinics maintain inflexible protocols for terminal gadget choice, other clinics rely more on affected person and parent input, combined with historic success charges for system types. Clinics that preserve very excessive caseloads for myoelectric devices, for example, will more than likely have far more expertise in becoming externally powered prostheses, in comparison with a clinic that may only see a handful of potential myoelectric candidates.
Discount cleocin gel 20 gm with mastercard
Resection of a calcaneonavicular coalition with muscle or fat interposition is indicated in a affected person younger than sixteen years of age who has a cartilaginous bar with no other coalitions present and no degenerative arthrosis acne light mask cheap cleocin gel 20 gm mastercard, and who has undergone unsuccessful nonsurgical therapy (513 skin care 08 purchase cleocin gel 20gm on line, 514) skin care reddit cleocin gel 20gm amex. The absence of degenerative changes in the talonavicular joint and calcaneocuboid joint ought to be ensured. In his evaluation of 30 specimens, the anterior aspect of the subtalar joint was totally spared in eight. The anterior aspect was partially changed in 7 of 30 specimens and fully changed in 15. This variation within the anterior portion of the subtalar joint associated to calcaneonavicular coalitions could end in some variation in outcome and positively relates to the extent and depth of the resection required to adequately deal with this downside. Failure to resolve signs with excision is commonly associated to inadequate resection at the time of the primary procedure (504). This coalition is positioned on the strain aspect of the valgus deformity of the hindfoot, and additional progressive flattening of the arch may occur following resection. Many of the ft with poor outcomes also had narrowing of the posterior aspect (indicating secondary ankylosis of the most important and most important facet of the subtalar joint) and impingement of the lateral process of the talus on the calcaneus. The unbiased affect of the dimensions of the coalition was not decided by this or any examine to date. These are, nonetheless, essentially the most goal standards for figuring out the resectability of a talocalcaneal tarsal coalition. The calcaneonavicular bar is approached via an Ollier incision on the dorsolateral floor of the foot. The incision may extend from the extensor tendons to the peroneal tendons in a pores and skin crease over the coalition (A). With experience, this incision could be relatively small when positioned instantly over the coalition. It is important that the initial incision be made through the complete layer of skin, subcutaneous tissue, and fascia overlying the extensor brevis muscle, without undermining the wound edges. The fascia of the extensor brevis muscle is opened and elevated proximally off the muscle itself. After exposing the proximal origin of the extensor brevis muscle, an incision is made into the fibrofatty tissue deep into the sinus tarsi. These parts of the fibrofatty tissue and the extensor brevis muscle are dissected distally as a unit, exposing the bar connecting the anterior end of the calcaneus and the navicular, in addition to the calcaneocuboid joint (B). This distally based flap of soft tissues will either act because the interposition materials or will cover a free fats graft that can be utilized instead interposition material. A hemostat or suture could be positioned on the fibrofatty tissue to retract it and the extensor brevis muscle out of the way without damaging the muscle. The commonest error is to excise too little bone from the plantar-medial nook of the bar. Good exposure of the sinus tarsi, the place the calcaneus and the talus are in shut approximation, will aid in directing the osteotome within the correct path. After the bar is excised, the surgeon ought to have the power to see a distinct gap separating the anterior facet of the calcaneus and the navicular. In addition, examination of the foot should affirm that subtalar movement is restored. It should be attainable to displace the origin of the extensor brevis muscle into this gap between the calcaneus and the navicular that was created by removing of the bar. A heavy absorbable suture is threaded through the end of the extensor brevis muscle, and an extended, heavy, straight Keith needle is threaded onto every end of the suture. If the extensor brevis is used because the interposition material, two straight Keith needles are handed through the hole that was left by the excision of the bar and out through the pores and skin on the medial side of the foot. A forceps is used to guide the muscle deep into the defect whereas the suture is pulled through and tied over the button on the medial aspect of the foot. This should result in the muscle being interposed between the reduce ends of the calcaneus and navicular. Placing each sutures on one needle lessens the chance that a nerve or other construction shall be trapped between the two sutures. Alternatively, a free fat graft from the buttocks or elsewhere in the extremity can be obtained for use because the interposition material. The wound is closed with interrupted absorbable sutures in the deep layer of muscle fascia and subcutaneous tissue that was rigorously preserved initially of the operation. After the forged is eliminated, the patient remains nonηeight bearing on the operated foot for a further 3 to four weeks while performing energetic range of movement workout routines multiple times per day. A: Oblique radiograph of the foot of a 10-year-old lady with a 1-year historical past of foot pain demonstrating an incomplete calcaneonavicular coalition. C: One yr after resection of the coalition, no reformation of the bar has occurred. However, valgus deformities in excess of 21 levels required postoperative bracing and had compromised outcomes. Degenerative arthrosis associated with either coalition is considered to be a contraindication to resection, but that analysis is difficult to set up. That concept has been changed with the assumption that the beak represents a traction spur, because it recedes with successful resection of the coalition. Its presence is, therefore, not a contraindication to resection (517, 518, 520, 521). The incision should extend from the prominence of the navicular to the realm posterior to the posterior aspect of the subtalar joint. The flexor hallucis longus tendon, which runs just beneath the sustentaculum tali, can also be retracted out of the finest way. The posterior tibial tendon can be identified working above the sustentaculum tali. To expose the coalition and define its anterior and posterior boundaries, an incision is made within the periosteum barely to the dorsal aspect of the prominence, which is the sustentaculum tali and the middle facet coalition. This must be done with care as a result of, although this periosteum is commonly skinny, it is going to be essential to approximate it later to maintain the fat graft in place. This dissection should be carried far sufficient anteriorly and posteriorly to identify regular joint space. The medial side of the coalition and its anterior and posterior boundaries are actually identified. The lateral extent of the coalition may be judged from the preoperative computed tomographic scans. Some slight movement could additionally be noticed within the normal components of the joint which may be exposed. To accomplish this, a small osteotome can be used to shave off thin layers of bone until the fibrous or cartilaginous coalition is recognized. The removing of synchondrosis and bone is continued until the 2 matching articular surfaces of the anterior aspect and those of the posterior side are seen. A laminar spreader may be inserted into the resection cavity to gently distract the subtalar joint. There must be little resistance to vertical distraction of the anterior and posterior sides.
Buy discount cleocin gel 20 gm online
A short-leg strolling cast is utilized for 2 extra weeks while the affected person gradually resumes full weight bearing skin care brand names buy 20 gm cleocin gel amex. The incision for the calcaneal lengthening osteotomy may be either an indirect Ollier kind of incision that crosses the sinus tarsi (A) acne like rash on face buy 20gm cleocin gel mastercard, as advised by Mosca (237 acne brush cleocin gel 20 gm,238), or a transverse incision instantly above the peroneal tendons, as originally described by Evans (236) (B). After the incision is deepened by way of the skin, the superficial peroneal and sural nerves are recognized, retracted, and guarded. The peroneal tendons are launched from their sheaths and the septum between them is resected. The calcaneocuboid joint ought to be identified by its landmarks however not opened; its capsule is important in offering stability to the anterior calcaneal fragment. The aponeurosis of the abductor digiti minimi is divided transversely 2 cm proximal to the calcaneocuboid joint. The gentle tissues are elevated from the undersurface of the isthmus of the calcaneus utilizing a Joker elevator or Crego retractor. After the osteotomy is performed and while holding the foot within the absolutely everted (flatfoot) place, a 2-mm clean Steinmann pin is inserted retrograde from the dorsolateral aspect of the forefoot throughout the calcaneocuboid joint stopping at the osteotomy. This pin is extraordinarily necessary as it prevents subluxation of the calcaneocuboid joint which may in any other case stop full deformity correction. Mosca (237,238) believes that the exit level should be between the anterior and center sides of the subtalar joint. To determine this, a Freer elevator is slid throughout the isthmus of the calcaneus to the medial side the place the center aspect is encountered. Slowly probing anteriorly, the surgeon will find the interval between the anterior and middle facets. It is to be famous that the airplane of this osteotomy is neither perpendicular to the lateral border of the foot nor parallel with the calcaneocuboid joint. Passing over the dorsum of the calcaneal isthmus, a Joker elevator is positioned within the interval between the anterior and center aspects. These instruments are used to establish the trail of the osteotomy and to protect the delicate tissues from the sagittal saw or osteotome. These will be used as pleasure sticks to distract the osteotomy when the graft is inserted. With it in place, the foot is inspected to make certain that the desired quantity of correction is achieved. The navicular and anterior calcaneal fragment move as a unit plantar-medially around the talar head because the osteotomy is opened. The osteotomy is held open by the 2 Steinmann pins whereas a trapezoidal tricortical iliac crest graft is inserted. This ought to be placed in order that a minimum of one cortex of the graft is involved with the cortices of the calcaneal fragments to give structural stability to the construct. The beforehand inserted 2-mm clean Steinmann pin is advanced retrograde by way of the graft and into the posterior calcaneal fragment. Other features include minimal bursal thickening over a relatively small medial eminence, and a great range of movement and an absence of degenerative modifications within the first metatarsophalangeal joint. Hallux valgus and firstγecond intermetatarsal angle: (A, B) axis of proximal phalanx; (C, D) axis of first metatarsal; (E, F) axis of second metatarsal. However, the overwhelming majority of evidence supports the conclusion that juvenile hallux valgus is attributable to structural abnormalities of the bones and joints (379, 380, 384), however is negatively influenced by constricting footwear. Flatfoot deformity and ligamentous laxity have been reported to be risk elements for the development of hallux valgus, in addition to its recurrence following surgical correction, by numerous authors (385ͳ87). The association of juvenile hallux valgus with the length of the first metatarsal is also controversial. An excessively long (379, 385, 390), as nicely as an excessively quick (391), first metatarsal has been implicated within the incidence, severity, and recurrence of juvenile hallux valgus deformity. Coughlin (379) has recently supplied information exhibiting that the relative lengths of the first and second metatarsals in children with juvenile hallux valgus are statistically much like the traditional inhabitants. The distal articular floor of the primary cuneiform is normally transverse; nevertheless, an oblique orientation of this joint might predispose to a varus deformity of the first metatarsal (387). The literature is inconsistent in figuring out an affiliation between adductus of all of the metatarsals and juvenile hallux valgus (379). X and Y: extent of metatarsal articular surface; X and Y: extent of proximal phalanx articular surface. As the deformity of hallux valgus progresses, the flexor tendons and sesamoids sublux laterally; the adductor of the good toe inserting on the proximal phalanx will increase the deformity, and eventually, once the hallux valgus deformity is current, the abductor hallucis with its medial insertion on the proximal phalanx has no capability to adduct the great toe. Piggott (395) believed that juvenile hallux valgus deformities with congruous joints have been stable and less more likely to progress than these with subluxation. Joint incongruity results in progressive deformity and degenerative arthrosis at an unpredictable fee. The form of the primary metatarsal could also be an etiologic issue within the development of juvenile hallux valgus. The articular cartilage on the distal finish of the primary metatarsal usually aligns almost perpendicular with the long axis of the bone. Lateral deviation, or orientation, of the articular cartilage might exist, thereby effectively creating a really distal valgus deformity of the metatarsal. Treatment may be divided into those strategies that relieve ache and those that relieve pain by way of deformity correction. There is only one report indicating a potential nonoperative means for correcting hallux valgus deformity. Conservative measures will relieve signs without correcting deformity in most patients with juvenile hallux valgus. Shoes with an sufficient toe field, a soft upper, and a low heel are more than likely to present pain aid. An arch assist can be utilized to lower the tendency for valgus eversion of the hindfoot. When considering buy of a pair of footwear, the right shoe ought to be turned upside down and pressed against the sole of the left foot (and vice versa). One ought to be in a position to see the sole of the shoe extending beyond each side of the forefoot when viewed from above. The weight-bearing foot can additionally be traced on a bit of paper and in contrast with the define of the shoe. Poor outcomes with excessive complication rates have been persistently reported in 30% to 60% of instances of surgery for juvenile hallux valgus (385, 399ʹ02). Coughlin (379) and others (391, 402) have performed successful surgical reconstruction with few complications in adolescents with juvenile hallux valgus with open development plates. Surgery, with its identified risks and complications, could have a deleterious effect on future efficiency. All parts and elements of the deformity have to be analyzed clinically and radiographically. The principle is to correct all elements of the deformity at the site(s) of deformity with out creating compensating deformities.
Order cleocin gel 20gm without a prescription
Reports of using triple innominate osteotomy to treat Perthes illness have begun to floor in the literature (408 acne treatments that work cheap cleocin gel 20gm on line, 409) skin care hospital in chennai discount cleocin gel 20 gm mastercard. This procedure za skincare order 20gm cleocin gel free shipping, originally introduced for the treatment of developmental hip dysplasia, is theoretically higher able to cover the deforming femoral head. Only longer follow-ups will let physicians know if it will supply better long-term outcomes compared with more generally utilized osteotomies. Recently, reports have been printed advocating the usage of hip distraction (arthrodiastasis) for durations of four to 5 months, with or with out soft-tissue release, in older children with Perthes illness (410, 411). The author has considerations in regards to the effect of pin tract contamination on the long run consequence of complete hip substitute in sufferers treated by this method. A judgment in regards to the usefulness of these procedures will have to await additional follow-up. Regardless of the tactic of containment chosen, any episode indicative of loss of containment, similar to recurrent ache or loss of vary of motion, must be handled aggressively with relaxation, traction, and reassessment of containment clinically and possibly radiographically. Treatment Options in the Noncontainable Hip and the Late-Presenting Patient with Deformity. Patients presenting with deformity in the later phases (reossification) of the disease, these with noncontainable deformities, and folks who have lost containment after undergoing both surgical or nonsurgical containment procedures current a management challenge. These sufferers often demonstrate hinge abduction on arthrography and have a particularly poor prognosis without extra remedy (193, 208, 209, 246, 348, 412). They usually present with persistent ache, shortening of the concerned extremity, and a fixed deformity, usually 10 to 15 levels of fixed flexion and 15 to 20 levels of fixed adduction (246, 412). In patients in the active stage of the disease regardless of their age with a noncontainable hip or patients with a painful hip after therapeutic who reveal hinge abduction, abduction osteotomy must be thought-about. In addition to altering the relation of the femoral head to the acetabulum, valgus osteotomy of the hip lengthens the leg and lowers and lateralizes the higher trochanter. Many hips suitable for valgus osteotomy also have a brief femoral neck, and the lateralization of the shaft tends to lengthen the neck. This scenario typically requires the modification of present units by bending, to avoid medialization of the femoral shaft or by shortening of the blade, of the blade plate units used for adults. The wound is normally fairly dry after the osteotomy is secured, and in our experience little drainage is collected in the suction canister. How dependable are the parents and youngsters in the following directions about activity? Adolescents are often massive enough to enable glorious fixation and rarely want a solid. On the other hand, youthful youngsters are often greatest immobilized for six weeks in a single-leg spica forged. Depending on circumstances, the cast may end above the knee and crutch strolling can be permitted. The preliminary results with this modality of treatment indicate improvement in limb length, lower in limp, and improvement in operate and vary of movement (412). This procedure could additionally be applied in either the lively or the late stage of the illness, when arthrography demonstrates that the congruency of the joint is improved by the prolonged adducted place. This modality of therapy permits for realignment of the congruent place of the hip in the impartial weightbearing place. The simplest approach is resection of a laterally primarily based wedge, by which a triangle of bone is faraway from the intertrochanteric area. How the wedge is made is dependent upon the kind of fixation used, and the wedge is designed to produce interfragmentary compression (416). If the 130-degree angled blade plate is used, the base of the osteotomy (the distal cut) is inclined and the proximal reduce is horizontal (A). Compression throughout the osteotomy web site is provided by the varus stress on the proximal segment. If a 90-degree blade plate is used, the bottom of the osteotomy is horizontal and the interfragmentary compression is obtained by prestressing the plate (B). The most tough of the valgus osteotomies to perform is the osteotomy that lateralizes the distal fragment and that lengthens the femoral neck. Although preoperative planning with templates can be used, an easier methodology, which is definitely helpful for most valgus or varus osteotomies, is one which uses proper intraoperative positioning of the femoral head in relation to the acetabulum, whereas the osteotomy and fixation are achieved relative to the median and coronal planes of the patient. The affected person may be placed on a radiolucent desk or a fracture desk so that a great view of the hip joint is obtained (A). The leg is adducted till the femoral head is in the desired relationship to the acetabulum (B). Next, the chisel for the 90-degree fixation device is inserted perpendicular to the median plane of the body (B). Finally, an osteotomy is created that can permit the femoral shaft to be introduced again into the median plane of the physique and secured with the plate (C). With the leg held in the desired position, a Steinmann pin is introduced into the most superior portion of the higher trochanter to serve as a information for the chisel. This pin ought to be perpendicular to the median plane of the physique and parallel to the ground of the operating room, which must be the identical as the coronal aircraft of the affected person. The position of this is verified on the image intensifier, and the chisel is driven in just below the guide pin. This site should be perpendicular to the shaft of the femur and at the level of the proximal margin of the lesser trochanter. A mark in the cortex crossing the osteotomy site or a Steinmann pin in the anterior cortex distal and at proper angles to the osteotomy ought to be positioned as a reference for rotation. With the blade in place, the plate is rotated toward the shaft, while the shaft is pulled laterally with a large forceps. The idea of this is to drive the lateral edge of the proximal floor into the medullary floor of the distal fragment (A). It is at this level that eradicating a portion of the proximal fragment parallel to the blade aids in the reduction and increases the contact of the 2 osteotomy surfaces (B). If nonetheless more shortening is required, further bone is removed from the distal fragment. It is often desirable to add an extension to the osteotomy, depending on the medical and arthrographic findings. After the osteotomy is accomplished, the proximal fragment is allowed to go into flexion. Any different corrections are made at the identical time, and the shaft is then secured to the plate. An 11-year-old boy with bilateral Perthes illness had a painful left hip with marked limitation of abduction and synovitis (A). His arthrogram demonstrates maximal abduction (B) and 30 degrees of adduction (C). Results of the valgus osteotomy four months after the procedure utilizing a 95-degree angled blade plate (D). Lateral shelf acetabuloplasty can also be used in "salvage" conditions, including lateral subluxation of the femoral head, insufficient coverage of the femoral head, and hinge abduction associated with severe Legg-Calv鮐erthes disease (362, 406, 418ʹ23). The writer has been impressed with early results of this method in older sufferers within the early levels of Legg- Calv鮐erthes disease.
References
- Clark WR, Malek RS: Ureteropelvic junction obstruction: observations on the classic type I adults, J Urol 138:276, 1987.
- Pardee AB: G1 events and regulation of cell proliferation, Science 246:603n608, 1989.
- Beutler E, Nguyen NJ, Henneberger MW, et al. Gaucher disease: gene frequencies in the Ashkenazi Jewish population. Am J Hum Genet 1993;52:85.
- Van Bortel LM, et al. Artery Society, European Society of Hypertension Working Group on Vascular Structure and Function, and European Network for Noninvasive Investigation of Large Arteries: Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J Hypertens 2012;30:445-448.
- Lopes RD, Hafley GE, Allen KB, et al: Endoscopic versus open vein-graft harvesting in coronary-artery bypass surgery, N Engl J Med 361:235-244, 2009.
- Bakker J, Coffernils M, Leon M, et al. Blood lactate levels are superior to oxygen-derived variables in predicting outcome in human septic shock. Chest. 1991;99:956-962.