

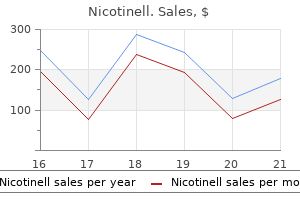
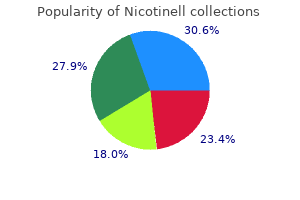
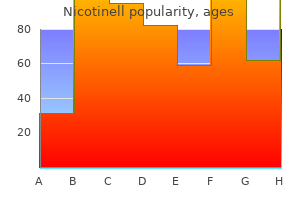
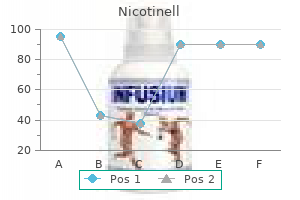
Nicotinell
Max S. Topp, M.D.
- Director
- Internal Medicine II
- University Medical Center II
- W?rzburg, Germany
Nicotinell dosages: 52.5 mg, 35 mg, 17.5 mg
Nicotinell packs: 1 packs, 2 packs, 3 packs, 4 packs, 5 packs, 6 packs, 7 packs, 8 packs, 9 packs, 10 packs

Buy discount nicotinell 35mg line
J Neurol Sci 233:15�19 quit smoking 8 years discount nicotinell 17.5 mg overnight delivery, 2005 Institute of Medicine: Gulf War and Health quit smoking research study cheap 35 mg nicotinell fast delivery, Vol 7: Long-Term Consequences of Traumatic Brain Injury quit smoking nicorette buy 52.5mg nicotinell with mastercard. Brain Inj 20:1335� 1344, 2006 Mild Brain Injury Langlois J, Rutland-Brown W, Wald M: the epidemiology and impact of traumatic mind injury: a brief overview. J Head Trauma Rehabil 21:375�378, 2006 Lee S, Wong M, Samii A, et al: Evidence for vitality failure following irreversible traumatic mind harm. Neurosurgery 39:510�514, 1996 Maddocks D, Saling M: Neuropsychological deficits following concussion. Am J Psychiatry 158:440�446, 2001 Marcoux J, McArthur D, Miller C, et al: Persistent metabolic disaster as measured by elevated cerebral microdialysis lactate-pyruvate ratio predicts continual frontal lobe brain atrophy after traumatic mind damage. Clin J Sport Med 10:235�238, 2000 McCrory P, Meeuwisse W, Johnston K, et al: Consensus assertion on concussion in sport, offered at the third International Conference on Concussion in Sport in Zurich, November 2008. Clin J Sport Med 19:185�200, 2009 McCullagh S, Oucherlony D, Protzner A, et al: Prediction of neuropsychiatric end result following delicate trauma brain harm: an examination of the Glasgow Coma Scale. J Neurol Neurosurg Psychiatry forty four:527� 533, 1981 McLean A, Temkin N, Dikman S, et al: the behavioral sequelae of head harm. Arch Phys Med Rehabil 89:1550�1555, 2008 Rapoport M, McCauley S, Levin H, et al: the role of injury severity in neurobehavioral end result three months after traumatic mind damage. Neuropsychiatry Neuropsychol Behav Neurol 15:123�132, 2002 Rapoport M, Kiss A, Feinstein A: the impression of major despair on end result following mild-to-moderate traumatic mind injury in older adults. Arch Phys Med Rehabil 84:1885�1894, 2003 Richardson J, Barry C: the effects on minor closed head damage upon human memory: additional proof on the role of mental imagery. Cogn Neuropsychol 2:149�168, 1985 Richardson J, Snape W: the consequences of closed head harm upon human memory: an experimental evaluation. J Affect Disord 19:237�241, 1990 Mooney G, Speed J: the association between delicate traumatic brain damage and psychiatric situations. Brain Inj 15:865�877, 2001 Mooney G, Speed J, Sheppard S: Factors related to restoration after mild traumatic brain injury. Neuroscience 136:971�989, 2005 Nakabayashi M, Suzaki S, Tomita H: Neural injury and restoration close to cortical contusions: a medical magnetic resonance spectroscopy study. J Neurol Neurosurg Psychiatry 31:299�306, 1968 Pagulayan K, Hoffman J, Temkin N, et al: Functional limitations and melancholy after traumatic brain damage: examination of the temporal relationship. Arch Phys Med Rehabil 89:1887� 1892, 2008 Paniak C, MacDonald J, Toller-Lobe G, et al: A preliminary normative profile of gentle traumatic mind harm diagnostic criteria. J Clin Exp Neuropsychol 20:852�855, 1998 Paniak C, Reynolds S, Toller-Lobe G, et al: A longitudinal study of the relationship between monetary compensation and symptoms after handled delicate traumatic brain damage. J Clin Exp Neuropsychol 24:187�193, 2002 Park E, McKnight S, Ai J, et al: Purkinje cell vulnerability to gentle and severe forebrain head trauma. J Neuropathol Exp Neurol 65:226�234, 2006 Ponsford J: Rehabilitation interventions after mild head harm. Curr Opin Neurol 18:692�697, 2005 Ponsford J, Willmott C, Rothwell A, et al: Factors influencing consequence following mild traumatic mind harm in adults. J Clin Exp Neuropsychol 21:620�628, 1999 Schneiderman A, Braver E, Kang H: Understanding sequelae of injury mechanisms and gentle traumatic mind damage incurred during the conflicts in Iraq and Afghanistan: persistent postconcussive symptoms and posttraumatic stress dysfunction. Am J Epidemiol 167:1446�1452, 2008 Schoenhuber R, Gentilini M: Anxiety and melancholy after mild head damage: a case control examine. Am J Psychiatry 144:93�96, 1987 Sigurdardottir S, Andelic N, Roe C, et al: Cognitive restoration and predictors of useful outcome 1 year after traumatic mind damage. Brain Inj 15:935�945, 2001 Silver J, McAllister T, Arciniegas D: Depression and cognitive complaints following mild traumatic mind damage. J Head Trauma Rehabil 5:1�10, 1991 Stein M, McAllister T: Exploring the convergence of submit traumatic stress dysfunction and delicate traumatic brain damage. J Psychosom Res sixty three:637�645, 2007 Stulemeijer M, van der Werf S, Borm G, et al: Prediction of favourable recovery 6 months after mild traumatic mind harm. Brain Inj 12:77�80, 1998 Teasdale G, Jennett B: Assessment of coma and impaired consciousness: a sensible scale. J Neurotrauma 22:42�75, 2005 Thurman D, Alverson C, Browne D, et al: Traumatic Brain Injury in the United States: A Report to Congress. Neurosurgery sixty two:1286�1295; discussion 1295� 1296, 2008 Vaishnavi S, Rao V, Fann J: Neuropsychiatric issues after traumatic mind injury: unraveling the silent epidemic. Psychosomatics 50:198�205, 2009 van Reekum R, Cohen T, Wong J: Can traumatic brain injury trigger psychiatric disorders J Clin Exp Neuropsychol 29:585�598, 2007 Vanderploeg R, Belanger H, Curtiss G: Mild traumatic mind harm and posttraumatic stress dysfunction and their associations with health signs. Ann Clin Psychiatry 12:131�135, 2000 264 Textbook of Traumatic Brain Injury Zaloshnja E, Miller T, Langlois J, et al. Brain Inj 7:147�152, 1993 Whelan-Goodinson R, Ponsford J, Johnston L, et al: Psychiatric issues following traumatic mind damage: their nature and frequency. J Head Trauma Rehabil 24:324�332, 2009 Whittaker R, Kemp S, House A: Illness perceptions and end result in mild head injury: a longitudinal examine. Geneva, World Health Organization, 1992 World Health Organization: International Statistical Classification of Diseases and Related Health Problems, tenth Revision. The development of posttraumatic epilepsy further complicates recovery by the use of the bodily and psychological penalties of seizures in addition to the medicines used for his or her therapy. Epidemiology of Posttraumatic Epilepsy Trauma is amongst the most common identifiable etiologies for the development of epilepsy, responsible for 20% of symptomatic epilepsy (Agrawal et al. Young adults and people with army accidents have the very best incidence of posttraumatic epilepsy (Agrawal et al. The time period posttraumatic epilepsy should rightfully be reserved for 2 or extra unprovoked seizures occurring after mind trauma, though in plenty of research a single seizure is considered synonymous with epilepsy. Timing of Posttraumatic Seizures the timing of incidence of seizures after brain trauma is necessary in prognostication and has been categorized in research as instant, early, and late. Immediate seizures occur inside the first 24 hours of injury, early seizures inside the first week, and late seizures beyond 1 week (Agrawal et al. Immediate seizures, together with contact seizures in the intervening time of harm, are often not included in epidemiological studies of posttraumatic epilepsy. Children are significantly prone to expertise instant seizures, with as a lot as 94% of those who experience seizures having them in the first 24 hours (Hahn et al. Such seizures have generally been thought-about to not carry a high threat of the development of epilepsy. However, Kollevold (1978) reported that both quick and early seizures increased the danger of late seizures. Children also have a 50%� 100% greater threat of early seizures than adults with comparable injuries (Annegers et al. Most research have reported an identical elevation of epilepsy danger with the prevalence of early seizures, with a lifetime incidence of epilepsy as excessive as 25% (Jennett 1975; Temkin 2003). In just about all studies late seizures carry a much greater danger of epilepsy (Agrawal et al. In phrases of timing, roughly 90% of posttraumatic seizures occurring throughout the first month will occur in the first week (Jennett 1975). Such seizures may be because of perioperative events, edema, and metabolic components (Agrawal et al. Of those that develop posttraumatic epilepsy, 80% expertise their first seizure throughout the first 12 months and 90% by the tip of the second 12 months (Da Silva et al. However, 15%�20% of sufferers might expertise their first seizure past 2 years (Agrawal et al.
Purchase nicotinell 52.5 mg with visa
The collateral ligaments are repaired quit smoking techniques buy nicotinell 17.5mg with amex, imbricated quit smoking exercise cheap nicotinell 35mg on-line, or reconstructed as could also be required to restore stability (especially against ulnar deviation quit smoking cartoons generic 35mg nicotinell with visa. If the capsule is sufficiently sturdy, repair it with interrupted 3-0 absorbable suture. After final implant placement, the collateral ligaments are repaired by way of drill holes placed in the metacarpal. This is most important for the radial collateral ligament in rheumatoid arthritis. Detachment of the collateral ligaments at their insertion is required for optimum exposure and visualization (may be repaired again to volar plate at closure). Bone Pntparation � Using an oscillating saw, take away the condyles of the proximal phalanx head, staying perpendicular to the lengthy axis of the bone in both the posteroanterior and lateral planes. Use awls, hand reamers, and broaches to prepare the medullary canals of the proximal and center phalanges. Split the central slip longitudinally and elevate it radially and ulnarly, taking care not to injure the central slip insertion and create an iatrogenic boutonnil! Other options are as follows: � the longitudinal split of the extensor mechanism could additionally be carried to one or both sides of the central slip insertion for its safety (. A distally primarily based triangular flap of the extensor mechanism is created; this provides glorious joint publicity and the extensor mechanism is later repaired (. The remaining portion of the procedure is much like that described as a half of the volar method. Note the silicone implant arthroplasties for the proximal interphalangeal joints of the index and lengthy fingers as nicely as the fusions of the distal interphalangeal joints of the long and ring fingers. Create dorsal drill holes at the origin of the correct collateral ligaments to be used for restore. Dynami~ extension (daytime) splints, stati~ extension (nighttime) splints, or each are fabrkated. Adjustments to the splints are ~ommonly required because the en~apsulation pro~ess and the healing pro~ess progress. Total joint movement is decided by the preoperative motion however typkally averages about 45 levels. Patients with a boutonniere or swan-ned deformity are most likely to be undanged or worse in regard to their deformity Metacarpophalangeal joint arthroplasty in rheumatoid arthritis: a loog- term assessment. Proximal interphalangeal joint silicone alternative arthroplasty: medical outcomes using an anterior strategy. Silicone implant arthroplasty in sufferers with idiopathic osreoarthritis of the metacarpophalangeal joint. Loog-rerm evaluation of Swanson implant arthroplasty in the proximal inrerphalangeal joint of the hand. Degenerative arthritis may occur after trauma or an infection or could come up as an idiopathic course of. Radial inclinations of the metacarpals and wrist joint destruction often leads to an ulnar translation of the whole carpus. Subchondral bone stiffens and periarticular new bone formation happens, which leads to restricted joint motion and pain.! Mild shows might go undiagnosed for years, while severe shows could progreas to speedy joint destruction in the third or fourth decade of life. Although the order of reconstruction is controversial, deficits of the shoulder, wrist, and elbow must be addressed earlier than addressing hand conditions. Extensor tendon or flexor tendon ruptures should be handled earlier than considering implant arthroplasty of the hand. Grade 1: No distinction in joint line opening compared to the contralateral joint Grade 2: Notable opening of the joint line in comparability with the contralateral joint, but a stable "endpoint� is reached Grade 3: Complete opening of the radial or lateral joint line with valgus or varus stress. This includes functioning flexors and extensors as properly as intact radial and ulnar collateral ligaments. Relative contraindications embrace the presence of a static swan-neck8 or boutonniere deformity. Patients should also bear in mind that heavy lifting or gripping have to be avoided indefinitely. If potential, dissect the sagittal bands from the capsule and protect them in order that the extensor tendon may be relocated and the sagittal bands imbricated on the finish of the process in order to keep a centralized extensor tendon place. If the joint is irreducible, it may be essential to release one or both collateral ligaments from their origins. Tag the ends of the collateral ligaments for later ~ pair to their tuberosity origins. A second minimize � oriented forty five levels proximally and volarly removes the rest of the metacarpal head, retaining the collateral ligament origins. Perform sequential broaching for the metacarpal until a correct fit has been attained. This supplies a better moment arm for the radial intrinsic and extrinsic tendons to compensate for ulnar drift. A plastic impactor with a concave floor aids insertion of the metacarpal proximal trial component. Once the trial parts are inserted and the joint is lowered, verify component frt and place utilizing a picture intensifier. Closure and Soft Tissue Balancing � After hardening of the cement, tighten the collateral ligaments or reattach them to the tuberosity of the metacarpal head with nonabsorbable suture. Cement fixation of 1 finger at a time is advisable if pe> sitioning is difficult. After the cement has cured, check passive range of me> tion to ensure adequate vary with out impingement or prosthetic binding. Protect the radial and ulnar collateral ligaments utilizing small Hohmann retractors while bringing the articular floor of the middle phalanx into view. While protecting the volar plate with a small retractor, use a 2-mm burr to help in making a small again cut (or chamfer cut to settle for the posterior aspect of the prosthetic condyles of the proximal phalangeal component. Make a perpendicular osteotomy on the base of the mi~ die phalanx with a small rongeur and remove no more than 1 to 2 mm of bone. In these circumstances, the prosthetic stems and flanges are merely coated with cement. The patient leaves the operating room with a sterile dressing, splinted in extension. Failure to use appropriate-sized implants could result in subsidence of the implants and posterior cortical impingement of the phalanges. If there was ulnar deviation before surgery, the fingers should be placed in 10 levels of radial deviation. A static rest or nocturnal splint capable of holding the fingers in the corrected place is used for 4 to 6 weeks. Better results have been obtained with arthroplasties carried out by way of a dorsal approach quite than the volar strategy. Range of movement at follow-up averaged -14 levels of emnsion and 61 levels of flexion. A distally based dorsal and triangular tendinous flap fur direct access to the proximal inrerphalangeal joint.
Discount nicotinell 35 mg line
Itching could be brought on by pesticides used 3 Inadequate or inappropriate therapy - Where one or two functions of the insecticide tried Young head lice seen following the first utility of insecticide could have hatched from eggs after the primary application quit smoking key chain discount nicotinell 35mg line. Determine if head lice seen are: Young (pin head size): or use "Wet Combing" remedy routine quit smoking 90 days ago will thc show in hair order 35mg nicotinell mastercard. Advise that a full "Wet Combing" routine is adopted to deal with head lice and then to use "Wet Combing" weekly to detect and forestall re-infections quit smoking insomnia trusted 17.5 mg nicotinell. Bed bugs hide and lay their eggs on the ground by the wainscoting cracks and crevices in beds and mattress frames, bedclothes, mattresses, bedsprings, furniture, curtains, soft furnishings, beneath wallpaper and skirting boards and so forth. Their chunk usually offers rise to a hard, whitish swelling that leaves a darkish, pink spot surrounded by a reddened area. To eradicate the mattress bugs it might be necessary for Pest Control to deal with the contaminated area with insecticide on a couple of occasion. Depending on the extent of the infestation, the Infection Control Team could advise that some furnishings get replaced or that room redecoration is required. If the service person is in single accommodation, they will need to switch to one other bedroom. All of the mattress linen is sent to the laundry service or washed inside out on the hottest wash it might possibly tolerate and tumbled dried. You need to consider if clothes, toys and loose articles or such like from the ground could also be infested. A prescription of antihistamines might assist management pores and skin itchiness from the insect bites. Knowledge this coverage is to be used at the aspect of Standard Precautions, Spillages, Waste Disposal and Safe Use and Disposal of Sharps policies. These viruses can be transmitted when a needle or sharp object contaminated with infected blood or body fluid penetrates the skin within the well being care setting. Hepatitis B and C infections might clear up utterly or result in a continual carrier, which may progress to cirrhosis of the liver. Care of service users with blood-borne viruses Using sterile needles, avoiding unsafe sexual practices and carrying protective equipment when dealing with blood/body fluids achieve prevention of transmission of blood borne viruses. The transmission of blood borne viruses, from patient-to-patient, or affected person to health care employees can have severe consequences not just for the individual infected but in addition for the trust because of well being and security laws. In spite of guidance and schooling, many health care staff continue to be uncovered to blood borne viruses from needlestick, sharp accidents and mucosal exposure, (Evans et al 2001). Hepatitis B is a preventable disease and the Department of Health recommends that staff at risk should be vaccinated. Gloves should be worn when giving first aid, eradicating or changing wound dressings and dealing with soiled laundry. Four diseases could be transmitted from person to person and have a high mortality price: Lassa fever; Crimean/Congo Haemorrhagic fever; Ebola and Marburg viruses. Accidental inoculation or contamination of mucous membrane or damaged pores and skin by physique fluids has a potential threat of transmission. Transmission the preliminary an infection is acquired through contact with urine from the multi-mammate rat. Person to individual unfold is by way of needlestick damage or close contact with oral secretions. Incubation period the incubation interval is 3 - 17 days Clinical traits Fever (lasting 6-30 days); headache; shivering and a sore throat are frequent. Swelling of the face and neck, vomiting and diarrhoea can sometimes be adopted by renal and circulatory failure, with bleeding into the pores and skin and mucosa. Clinical Characteristics High fever; rigors; headache and myalgia develop, followed by vomiting and severe diarrhoea. Transmission Infection may be acquired from monkeys, and person to particular person by way of blood/body fluids. Clinical Characteristics Fever; rigors; headache and myalgia, with diarrhoea and vomiting; Rash and spontaneous bleeding are widespread. Transmission the infection is transmitted by a tick chew however could be acquired by contact with blood. Clinical Characteristics Fever; rigors; headache and limb pain develop, followed by vomiting. Page 137 Treatment Some antivirals could additionally be beneficial but remedy is mostly supportive. Management of Suspected Cases Service customers must be placed in minimal, average or high danger teams on suspected prognosis of viral haemorrhagic fever. Early in the illness, standard infection management precautions are adequate safety towards transmission of infection. Unless the diagnosis can be rapidly excluded, the service person must be referred to a specialist centre. The admitting doctor should formally notify suspected or confirmed cases of viral haemorrhagic fever to Public Health England. Minimum Risk Person has a fever however has not been in a identified endemic area or from endemic space. Moderate Risk Person has a fever and is from an endemic space within 21 days earlier than onset of signs, or from adjacent area with severe illness, organ failure or unexplained haemorrhage. High Risk Person has a fever plus: From an endemic space within three weeks before sickness and in a house for more than 4 hours where there was a suspected case or has nursed unwell, febrile sufferers or had contact with body fluids or dead physique of suspected case; previous moderate danger but developed organ failure and/or haemorrhage. Not from endemic space however cared for suspected case, contact with physique fluids or tissues or dealt with clinical specimens suspected to include the virus. Infection Control will provide further advice and assist about cleansing the room the service consumer has been in. Useful Contacts/Information Infection Control �020 3317 3487/078 1018 0774 or 020 3317 3353/078 8766 1854 Infection Control Doctor- 0845-155-5000 Ext 9516/99114 *Out of hours contact 0845-155-5000 and ask to be put via on to Professor Wilson or the Microbiologist on name North East and North Central London Health Protection Team-020 7811 7100 Occupational Health: 0203 317 3350 6. Chickenpox usually confers lifelong immunity, though the virus persists in a latent form within the sensory nerves. Reactivation of the latent varicella virus in later life leads to shingles (Herpes zoster). Clinical Features Chickenpox Characterised by a blister-like itchy rash, seems initially on the face, scalp and trunk, but can unfold over the complete body. Other symptoms which can precede the rash by 48 hours include general malaise, fever and headache. Shingles the virus causes severe pain and itching adopted by the event of blister-like lesions, occurring on the web site of the affected sensory nerve, typically causing a striplike sample on one side of the physique. Transmission Chickenpox Chickenpox is transmitted through direct person to person contact, by way of airborne unfold of respiratory droplet nucleii, and vesicle fluid or via contact with infected articles similar to clothes and bedding. Transmission can happen via direct contact with exudate from wet lesions or airborne through vesicle fluid in disseminated shingles. Infectious Period Chickenpox probably the most infectious period is from one to two days before onset of the rash and continues for one week after onset or until all lesions are dry and have crusted. Page a hundred and forty Testing Adults suspected of having chickenpox require a viral swab taken from a wet vesicle. Infection Control Precautions Service customers with chickenpox or shingles should solely be attended by workers identified to be immune.
Purchase nicotinell 52.5 mg mastercard
I agree not to quit smoking 2 years ago still anxiety cheap nicotinell 52.5 mg with visa share quit smoking medication safe 35mg nicotinell, sell or commerce my prescribed medicine for cash quit smoking symptoms nicotinell 17.5mg free shipping, items and/or companies. I will also safeguard my treatment from theft, loss or potential misuse (do not depart your medicine the place others can access it. I understand that if I violate any of the above conditions, my prescription for controlled substance medications could also be terminated immediately. If the violation includes acquiring controlled substance medications from one other particular person, or the concomitant use of non-prescribed illicit (illegal) drugs, it could even be reported to my physicians, medical facilities and acceptable authorities. I perceive that the main therapy goal is to scale back pain and enhance my ability to function and/or work. In consideration of this goal, and the truth that I am being given a potent medication to help me reach my objective, I conform to assist myself by the next higher heath habits: workouts, weight management, and avoidance of using tobacco and alcohol. I perceive that a profitable end result to my treatment will solely be achieved by following a wholesome lifestyle. I understand that the long-term benefit and disadvantages of continual opioid use have but to be scientifically decided and my therapy might change at any time. I understand, accept, and agree that there may be unknown risks associated with the long-term use of controlled substances and that my doctor will advise me of any advances on this subject and will make therapy changes as wanted. Zasler and his employees regarding psychological dependence (addiction) of managed substance medications, which I perceive is rare. Therefore, when I must stop taking the medicine, I should achieve this slowly and under medical supervision or I could have withdrawal signs. I conform to be treated with alternative methods, both drug or non-drug in nature, as they become out there, and on the recommendation of Dr. Zasler, even if my pain condition is modulated by the use of opioid treatment of any kind. I actually have read this doc and I fully understand its content material and the consequences of violating the phrases of this settlement which embrace potential discontinuation of prescription of managed substances by Dr. Zasler to the patient in query and potential termination of the physician affected person relationship. Patient Name (printed): Patient Signature: Date: the above phrases and circumstances have been discussed with, and understood by, the aforementioned patient: Date: Nathan D. The complexity of those components, not solely singly but in addition integrated into their influence on human habits, presents scientific assessment and therapy challenges in addition to methodological challenges for research (Sandel et al. Brain damage may produce sexual dysfunction at the genital stage in addition to adversely have an effect on expression of sexuality on the nongenital stage. To better comprehend the effect of mind harm on sexuality, one must first perceive the basic neuroanatomical pathways and neurophysiological mechanisms which may be concerned in the mediation of sexual function. Professionals must tackle the realm of sexuality as they do other useful areas of human "efficiency," together with mobility, activities of daily living, and bowel and bladder operate, to present a comprehensive method to the issue and reduce any resultant practical impairment. Abnormal and/or inappropriate sexual conduct typically impacts not only the affected person but additionally potentially his or her spouse, household, and/or caretakers. Attitudes regarding sex and sexuality often function obstacles to dealing with these important points in a structured, educated, and timely style (Johnson et al. By offering appropriate early intervention after trauma and appropriate follow-up, the skilled permits for higher adjustment to and therapy of postinjury sexuality issues. Masters and Johnson (1966) proposed a four-stage mannequin of sexual response, which they described because the human sexual response cycle. They outlined the 4 phases of this cycle as excitement/full arousal, plateau, orgasm, and backbone. They additionally were the primary to describe the phenomenon of the rhythmic contractions of orgasm in each sexes occurring initially in zero. In 1979, Kaplan added the concept of need to the model and condensed the response into three phases: need, arousal, and orgasm. First, it assumes that men and women have comparable sexual responses, and therefore it may lead to faulty conclusions about normal sexual conduct in girls. In 1997, Whipple and BrashMcGreer proposed a circular sexual response pattern for 397 398 Textbook of Traumatic Brain Injury girls. This idea is constructed on the Reed model, which comprises four phases: seduction (encompassing desire), sensations (excitement and plateau), give up (orgasm), and reflection (resolution) (Sandel et al. If the reflection phase is inadequately pleasing/arousing, then the lady may not have a desire to repeat the experience (Whipple and Brash-McGreer 1997). This model proposes that the female response cycle is much more advanced and circuitous than the male sexual response cycle, with the previous being significantly affected by psychosocial components similar to relationship standing, prior sexual experiences, and self-image. Peripheral nervous system Reticular activating system Afferent enter Efferent output Autonomic Sympathetic Parasympathetic Somatic Sexual Neuroanatomy Studies involving mapping of neuronal pathways in animal fashions have allowed scientists to develop a better understanding of the neuronal organization of central nervous system pathways involved in controlling numerous features of sexual functioning. Retrograde and anterograde tracing techniques have allowed the identification of many such pathways. Agents such as neurotropic viruses have been used as neuronal tracers to map complete networks of neurons in various animal models. More recently, functional imaging using positron emission tomography and functional magnetic resonance imaging has corroborated that a number of areas of the mind are activated during the sexual response (Rees et al. The multiple neural networks concerned are believed to embrace structures in the peripheral nervous system (both autonomic and somatic), brain stem, subcortex, and cortex. Cortical constructions, together with the frontal, temporal, parietal, and paralimbic cortex, are involved within the mediation of sexual operate. Stimulation of cortical buildings has produced genital hallucinations and erections (MacLean 1975). Certain cortical buildings, such as the piriform cortex, are in intimate reference to more primitive "sexual" systems, including the olfactory system. Animal research have shown that lesions in these areas might produce hypersexuality (Mesulam 1985). The frontal lobes are intimately involved with limbic and paralimbic structures via numerous neural connections. Inferomedial frontal damage could produce disinhibited and sexually inappropriate behavior, whereas dorsolateral frontal damage sometimes results in impaired sexual initiation (Walker 1976). Clinical expertise has revealed that sure patients with frontal damage demonstrate a compromised ability to fantasize that will impede masturbation. However, frontal involvement rather than laterality will be the more important factor (Horn and Zasler 1990). Research has demonstrated that lesions in the nondominant hemisphere could result in an array of deficits that compromise expression of sexuality, including dysprosody, visuoperceptual problems, and anosognosia. Additionally, the nondominant temporal lobe has been theorized to be the sexual activa- Sexual Dysfunction tion center for the brain (Cohen et al. Lesions in the dominant hemisphere might produce aphasias and apraxias, thereby compromising each communication and motor performance (Zasler 1991).
Buy generic nicotinell 17.5 mg on line
This often happens with people with frontal lobe accidents whose judgment could additionally be compromised or people with unstable medical situations corresponding to partially controlled seizures quit smoking questions discount nicotinell 17.5 mg online. Such families may block efforts at persevering with training quit smoking 6 months ago how should i feel nicotinell 35 mg cheap, job trials quit smoking oils nicotinell 52.5 mg lowest price, dating, or unbiased journey or living. An sincere dialogue of (usually parental) fears, coupled with a sensible discussion of the risks concerned (how practical the risks are and what steps could be taken to minimize them), is commonly helpful. For instance, a young woman with a extreme mind harm could additionally be interested in learning to journey independently between her house and a job trial website. More useful may be the strategy taken in principle #5 as outlined within the preceding part: elaborate and collaborate. Thus, the shopper might be guided to the work web site, then develop a map and set of steps to observe, then accompanied yet one more time however encouraged to make her personal choices, then accompanied however tailed solely, and so forth. Between each step, family members could be told how things went, and their consent could presumably be sought for taking the subsequent step. As with any program of deconditioning, the concept is to introduce at each step a objective that has a high probability of success and that arouses a minimum amount of hysteria. Allowing families to retain a way of management and safety in decisions about the injured particular person is a key idea in coping with unrealistic expectations. They are supposed to represent a few of the guidelines professionals can use when confronted with families whose goals are thought to be unrealistic. The different mistake is the other: to totally endorse the goal and reassure the woman that everybody will do everything potential to assist her obtain that goal. That would feed into her unawareness or denial of the implications of her deficits, or each, and set her up for a very devastating failure. Helping others, making struggling go away, or enabling a person to be taught and succeed might emerge as the driving forces. It is then potential to discover different profession or volunteer choices that can meet these wants and give the woman an experience doing them in a supervised setting. There are occasions when all else fails and the injured particular person and household insist on embarking on a path that the clinician deems unrealistic. Often, the reality is that the one way a family will confront the impossibility of a aim is to try it and fail. Setting up help services for the individual, keeping scientific contact as he or she begins the process, figuring out in advance what the troublesome areas will be, and having a contingency plan if all comes crashing down are the accountable scientific approaches. That way, the injured individual is protected as he or she involves phrases with what the clinician knew: that the goal was unrealistic. The one exception to allowing managed failure is when the worth of failure might be catastrophic when it comes to human or monetary well-being. Doctors, for example, can carry out restricted components of examinations underneath supervision. Principle #7: Be Prepared to Challenge Overprotective Families That Are Negatively Unrealistic. A separate downside, however one which falls underneath the class of unrealistic households, is the overprotective household that underestimates the capacities of the injured particular person. Psychological overlay can accumulate with time and will increase dysfunction, which usually reflects a complex interplay amongst organic, persona, and environmental factors. In many cases, a reliable, if subtle, mind damage underlies and drives the dysfunction, which is layered over with maladaptive psychological reactions, lots of which end result from inappropriate environmental responses (Kay 1992). An essential a half of any neuropsychiatric treatment of such complicated and troublesome instances is instant household involvement. Family responses and reactions to the obvious discrepancy between severity of harm and severity of signs can either induce or exacerbate a dysfunctional postconcussional syndrome. The family needs information and education concerning the nature and penalties of concussion and how to understand and assist the patient handle his or her signs. Also, any alienation that develops between the injured individual and the family must be healed. Often, this involves addressing old issues, either intrapersonal or throughout the household system, that are in fact contributing to the extreme stage of dysfunction. It is a mistake to see the apparent emotional overlay in such circumstances and dismiss the injured individual as malingering or the issues as purely psychosomatic ones. This ought to begin lengthy before the child is ready to return to school-soon after the accident has occurred whereas the kid is still within the acute or rehabilitation stage. When the kid is nearing discharge home, the parents need to ensure the rehabilitation staff is placing collectively suggestions for college wants and assist the group contact the suitable faculty personnel. Again, the parents should take the lead in contacting the varsity to work out these decisions. First, mother and father must take the initiative to meet frequently with the teacher(s) and repair suppliers inside the school. More frequent faceto-face or telephone contact with the classroom or research room or homeroom instructor is appropriate. For youthful kids, a communications book in which the teachers, mother and father, and therapists write notes, requests, and issues is commonly extremely useful. Assignments ought to be checked for readability so parents can monitor homework when essential. In our opinion, there are two circumstances during which medical professionals are justified in counseling families about authorized issues. First, not all private injury attorneys are subtle in bringing harm instances to settlement or trial. They might terribly underestimate the long-term disability of the particular person and simply not concentrate on what the long-term costs might be by means of misplaced wages and care wants. We have seen many households who have been counseled by lawyers to settle early for sums of cash grossly inadequate to care for the person in the lengthy term and who bitterly look again on their authorized recommendation wishing they knew then what they know now. Many kids "develop into" their deficits as the demands of faculty turn into greater and extra complicated and require more frontal lobe processing. However, the chance of ready to attempt the case is that other intervening occasions or variables over time could cloud the picture and make it rather more tough in later years to tease out the influence of an early injury. In our opinion, in cases by which the kid is simply too younger for the true effect of the harm to be decided, and if the family is being pressured to accept a small, quick settlement, there are ethical grounds for the clinician to discuss the legal points with the household and to urge dialogue of the problems with a lawyer as well. For instance, bodily therapists and occupational therapists within and outside the varsity ought to talk about their objectives and techniques to learn from one another. It is also important that there be an open line of communication between the college and physicians, especially round behavioral points, when seizures are suspected or when treatment is a matter. When dad and mom are involved in serving to with homework, which they usually are, they should discuss with academics and therapists which compensatory methods work greatest, and there should be consistency of implementation of those strategies across home and college settings in addition to consistency across internal school settings. This requires communication and drawback solving on the part of mother and father, teachers, and school professionals. Children are growing rapidly, particularly of their earlier years, whilst they endure recovery from the damage and the changing demands of recent academics, lessons, routines, and schools.
Cymbopogon afronardus (Citronella Oil). Nicotinell.
- What other names is Citronella Oil known by?
- What is Citronella Oil?
- How does Citronella Oil work?
- Worm infestations, fluid retention, spasms, and other conditions.
- Are there safety concerns?
- Dosing considerations for Citronella Oil.
- Preventing mosquito bites when applied to the skin. Citronella oil is an ingredient in some commercial mosquito repellents. It seems to prevent mosquito bites for a very short amount of time. Other mosquito repellents, such as those containing DEET, are usually preferred because these repellents last much longer.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96619
Purchase 17.5 mg nicotinell otc
Neuroradiology forty six:339�350 quit smoking jacksonville florida nicotinell 52.5mg visa, 2004 Tollard E quit smoking medication buy cheap nicotinell 52.5 mg on-line, Galanaud D quit smoking jitters discount 52.5mg nicotinell with mastercard, Perlbarg V, et al: Experience of diffusion tensor imaging and 1H spectroscopy for consequence prediction in severe traumatic brain damage: preliminary outcomes. J Neurotrauma 9 (suppl 1):S287�S292, 1992 Maruichi K, Kuroda S, Chiba Y, et al: Graded mannequin of diffuse axonal damage for learning head injury-induced cognitive dysfunction in rats. Functional imaging strategies promise to assist elucidate brain harm in these particularly difficult circumstances. These modalities symbolize the primary functional imaging methods out there right now. Activation scans are acquired throughout performance of a cognitive task, similar to memorization of words offered on a computer screen, which permits for assessment of perform in a (relatively) isolated domain when compared with a baseline scan. Use of an activation paradigm might assist to improve exercise in a sure community of buildings that are the major focus of examine. Few studies use pre- and postrecovery scans, which provide the benefit of permitting for comparability in the identical sufferers. The ultimate hope is that practical imaging will permit clinicians to more accurately assess mind impairment, higher predict potential for rehabilitation, and objectively measure restoration of perform. The actual contribution of these modalities to improvement in scientific care and consequence, nevertheless, is still more promise than reality. We start with a discussion of the way to evaluate the various forms of studies out there. Understanding the Literature As new techniques emerge, clinicians need to be ready to evaluate present analysis and critically evaluation published studies. Standardized scores of scans are the exception, although latest studies usually have a tendency to use quantitative approaches such as statistical parametric mapping. When affected person data are in contrast with information from regular control subjects, care must be taken to be sure that management topics are matched to the patient groups with regard to necessary variables similar to age, handedness, sex, and general health, all of which may affect brain blood move and metabolism. Matching for an equal level of physical trauma (orthopedic control) can be valuable. Finally, many injury-related components corresponding to bony harm, edema, changes in white matter integrity, and diffuse axonal damage might all complicate interpretation of useful imaging acquired utilizing any of the varied modalities (for review, see McAllister et al. This picture can be visually interpreted by a nuclear medicine specialist and/or analyzed statistically utilizing various software program packages. More credence should be given to studies performed with the newer triple-head cameras. Concentrations of this tracer are thus highest in areas receiving the most plentiful blood flow shortly following the injection and remain so for as a lot as 24 hours. Because of this long half-life, multiple scans can be acquired on a patient following one injection, which could be useful if the affected person moves. Intravenous radioactive tracer is injected into the patient a few minutes previous to scanning, preferably in a quiet, managed surroundings to decrease blood circulate adjustments due to anxiousness and presence of loud noise. The affected person ought to be able to lie nonetheless in a supine position in the scanner during the scan, up to half an hour. If the affected person is simply too agitated to remain still, sedation may be given after tracer injection, to decrease effects on the uptake and distribution of tracer. Because the affected person is uncovered to ionizing radiation with this technique, consideration should be given to the quantity and recency of prior scans using radioactive tracers. The identical scanner is used for imaging many physique methods, including brain, heart, bone, and lung. Before brain imaging, the affected person receives an intravenous injection of the radioactive tracer while mendacity in a darkened room. After a brief period within the darkened room to enable the tracer to distribute via the brain, the affected person is prepared to be scanned. The tracer distribution is stable for several hours, thus allowing a substantial time window for scanning to happen. The data are transmitted to a pc that produces tomographic images within the desired plane(s) of section. Interpretation is usually carried out by visible score of scans for abnormalities rather than with use of quantitative or statistical methods, introducing issues inherent in use of subjective, nonstandardized ratings. Comparisons of outcomes from different studies are difficult, as a outcome of some groups might report solely the presence of general abnormality whereas other groups might report variety of particular person lesions seen in each scan. The two are often extremely correlated, particularly in regular mind tissue, but an uncoupling of this relationship may occur after brain damage (Belanger et al. For example, if a ligand that binds particularly to one neurotransmitter sort is run, followed by a scan, and then an activation task is performed, a follow-up scan could potentially give information on how much ligand was displaced by the endogenous neurotransmitter, suggesting involvement of that system in the task. Instead, the scans had been interpreted individually, and useful results had been compared with these from structural modalities. Outcomes measured were neurological examination findings, postconcussive symptom checklist, and neuropsychological tests. However, it must be famous that little work has been carried out to elucidate the true relationship between an abnormal scan and goal end result measures, especially for instances of delicate hypoperfusion. Note the absence of move in the best anterior temporal and frontal lobes (foreground), leading to visualization of the left temporal and frontal lobes from the medial aspect. Merging blood move information with anatomical imaging additionally improves identification of areas of abnormality. A vital affiliation was discovered between basal ganglia hypoperfusion and postconcussive headaches. Hypoperfusion was also discovered within the left parietal and left temporal lobes (Atighechi et al. In one, a relationship was discovered between perfusion deficits and neuropsychological check efficiency in solely 14 of 120 comparisons (Weidmann et al. As noted by the authors, that is in keeping with recruitment of further areas to assist the attention management calls for of the duty. This resulted in severe trauma with lack of consciousness requiring neurosurgical interventions. A 24-year-old man had a motorcar accident with no lack of consciousness 10 years after a mild head injury. Shortly thereafter, the patient presented with extreme cognitive deficits, depression, agitation, aggression, and psychosis. Symptoms were sufficiently extreme to require prolonged psychiatric hospitalization. The most pronounced abnormality was reasonably lowered perfusion within the left parietal lobe near the posterior Sylvian fissure and in each temporal lobes. Mildly reduced perfusion was noted in the occipital lobes (left higher than right) and basal ganglia (particularly near the caudate heads). Some of these abnormalities are visible on each the sagittal and coronal photographs (arrows). Prior to remedy, motor task� associated increases have been present within the cerebellar hemispheres and vermis. Following completion of this system, task-associated will increase had been present within the vermis and anterior cingulate cortex but not the cerebellar hemispheres.
35mg nicotinell mastercard
Nonetheless quit smoking k2 buy nicotinell 52.5mg visa, there was no distinction between teams in discharge disposition (community vs quit smoking 3 months ago and still tired all the time buy generic nicotinell 52.5 mg. Therefore quit smoking sore throat discount nicotinell 17.5 mg on-line, though older patients required considerably longer and extra costly inpatient rehabilitation stays, their postdischarge tendencies have been comparable with these of youthful sufferers. Comparing psychosocial outcomes at 1 year postinjury in patients of varied ages, Rothweiler et al. Significantly extra patients older than 60 years required a change to a more supervised residing state of affairs than these youthful than 50 years. These research adopted patients with a predominance of reasonable to severe injuries. Rapoport and Feinstein (2001) compared subjects ages 60 years and older with these ages 18�59 years who had Cognitive Outcome Cognitive functioning exerts a considerable influence on functional independence in all age teams. Advanced age and related age-related medical sicknesses can lead to the prescription of quite so much of medicines, including psychoactive medicine, which increase the probability of drug-drug interactions (Zhan et al. In addition, older sufferers are inclined to require longer, extra pricey rehabilitative therapies, although they may benefit considerably from such interventions. An further concern is the concomitant use of psychoactive medicines and other drugs which will have an antagonistic effect on cognition. Acetylcholine innervation is extensively distributed all through the brain, mainly originating within the nucleus basalis of Meynert within the basal forebrain. Although no consistent loss of acetylcholine content is found in the brains of wholesome elderly people, cerebrospinal fluid levels of the degradative enzyme acetylcholinesterase are increased with advancing age (Hartikainen et al. These modifications could contain mind construction and performance that amplify the consequences of head trauma and reductions in physiological reserve that predispose older patients to secondary organ failure. Neurobiology of Aging the human mind achieves full maturity in the second or third decade of life, and age-associated histological changes develop after age forty years (Powers 2000). Agerelated cerebral atrophy might outcome from a lack of neurons, decrease in neuronal volume, and lack of synapses. Synaptic density declines with age, however the number of cortical neurons in lots of areas might stay stable by way of superior age (Haug and Eggers 1991). Neurotrophic elements similar to nerve development issue are essential to the traditional growth and maintenance of cholinergic neurons. Thus, the aging brain may be much less able to mount an effective regenerative response to mind trauma by way of neurotrophic components. Age-related cerebrovascular changes additionally lead to a progressive discount in cerebral perfusion and related reductions in regional cerebral metabolism (Tumeh et al. Loss of noradrenergic neurons in the locus ceruleus begins in the fourth decade of life and progresses in a linear fashion (Mann et al. Decreased exercise of the noradrenergic synthetic enzymes tyrosine hydroxylase and dopamine -hydroxylase additionally happens in the getting older mind (Powers 2000). Age-related lack of dopaminergic neurons in the nigrostriatal pathways begins in the fifth decade of life, resulting in as much as 35% loss by age sixty five (Mann et al. Neurochemical adjustments related to getting older Neurotransmitter Acetylcholine Location Nucleus basalis of Meynert Medial septal region Change or Brain ranges of the degradative enzyme monoamine oxidase-B improve with age, which may scale back monoaminergic transmission (Fowler et al. Density of type 1 receptors is decreased by as a lot as 70%, and type 2 receptor density is reduced by 20%�50% (Mendelsohn and Paxinos 1991). This reduction in central serotonergic functioning has been proposed as a possible contributor to the event of disturbances of temper and habits in elderly patients (Meltzer et al. Summary Aging mind demonstrates mild to moderate neuronal loss, with much of the volume loss attributable to neuronal and synaptic atrophy. This relationship was not affected by apoE genotype, multiple head accidents, or length of unconsciousness. The research was limited by a comparatively transient interview between baseline and follow-up of 2. Stratification by gender revealed that the surplus danger was current solely in males (odds ratio 2. A postmortem research discovered cortical -amyloid deposits in 30% of sufferers ages 8 weeks through 81 years who died inside four hours to 2. In this capacity, it could mediate neuronal repair, regeneration, and survival (Horsburgh et al. However, one study found no relationship between genotype and cognitive performing at 1 and a pair of years postinjury (Rapoport et al. A detailed and accurate history of preinjury bodily, cognitive, and psychological standing is essential. In this situation, a affected person might current with a number of weeks or months of progressive cognitive impairment. The affected person may either have had a witnessed or unwitnessed fall or other head trauma that was not thought to warrant medical consideration. Another presentation may contain the presence of orthopedic accidents resulting from a fall or cardiovascular pathology that precipitated a fall. These more emergent conditions may lead the first remedy staff to concentrate on acute stabilization, particularly in intensive care or surgical settings. Single-photon emission computed tomography or positron emission tomography may provide helpful information relating to alterations in regional cerebral perfusion and metabolism not detectable by structural neuroimaging. However, age-related changes within the mind may make interpretation of each structural and useful imaging results tough, significantly because cerebral perfusion could also be altered by regular aging (Tumeh et al. Age-related decline in memory efficiency is characterised by a fairly narrow range of impaired efficiency in acquisition and retrieval of newly realized info (Small et al. Moreover, decreased processing velocity in healthy aged subjects appears to be narrowly circumscribed and never attributable to general deficits in govt operate, inhibition, and working reminiscence (Salthouse 2000). Obtaining detailed collateral historical past of the presenting syndrome is crucial, as is a history of prior 456 Textbook of Traumatic Brain Injury cation unwanted side effects, significantly anticholinergic unwanted aspect effects. Attention must even be paid to physiological changes that alter the pharmacokinetics of medicines (see Table 29�5). Increases in body fat composition could increase elimination half-life of lipid-soluble medicines, whereas decreased serum proteins might result in increased bioavailability at equal serum ranges. Additional elements embrace decreased gastric emptying and ensuing slowed absorption and decreased renal and hepatic excretion. Age-related alterations in mind structure and performance require consideration of those adjustments when decoding results. However, in older sufferers, even more attention should be paid to age-specific elements that affect the physiology, psychology, and social circumstances of brain-injured sufferers. Environmental Interventions Environmental interventions should address age-associated sensory decline. Areas must be well-lit and free from extreme noise and other stimuli which will overwhelm and confuse the affected person.
Buy nicotinell 35mg with amex
The patient locations his or her arm on a desk with the wrist hanging off the sting whereas holding an empty bucket quit smoking 0001 cheap nicotinell 17.5 mg mastercard. The patient holds the bucket for 2 to three minutes and repeats the train twice daily in flexion and extension quit smoking 27 days order nicotinell 35mg free shipping. A protective covering (such as those used for recurrent nerve entrapments) to shield the dorsal ulnar nerve might reduce injury to the nerve quit smoking years ago buy nicotinell 35 mg with mastercard. Mechanical Testing of Distal Radioulnar Instability Repair: Ligament Reconstruction vs. Proceedings of the Annual Meeting of the American Academy of Orthopaedic Surgeons, Feb. Proceedings of the International Wrist Investigators Workshop, American Society for Surgery of the Hand. Studies on the tendinous comparttw:nts of the extensor muscles on the again of the human hand and their tendon sheaths. Comparison of the findings of triple-injection cineartbrography of the wrist with these of arthroscopy. The nerve is immediatdy uncovered after the opening incision and is susceptible Chapter 52 t Arthroscopic Dorsal Radiocarpal Ligament Repair -i-~ David J. U � Recognition of this situation and further analysis into therapy strategies is required. This would require adjustments in size far higher than any single fastened ligament might accomplish. It originates on the tubercle of Uster and moves obliquely in a distal and ulnar dir&tion to connect to the tubercle of the triquetrum. It can range its size by altering the angle between the 2 arms whereas sustaining its stabilizing effect on the scapholWlate joint during wrist. Of this subgroup one patient had Geissler stage 2 instability and one had a Geissler stage three or4 tear. Each successive stage denotes a longer standing or extra extreme condition, and this has a unfavorable impact on the prognosis. Positioning � the patient is positioned supine on the working desk with the arm kidnapped. The pre- and postoperative wrist movement was unchanged in four of those patients, with less than 15% lack of movement in the fourth affected person. Two had no pain (with wafer resection), two had occasional gentle ache, and three had chronic reasonable pain. Immunohistochemical evaluation of wrist ligament imu:rvation in relation to their structural composition. Bioou:chanical analysis of the ligamentous stabilizers of the scaphoid and lunate, half Ill J Hand Surg Am 2007;32A:297-309. The incidence of dorsal radiocarpalligaou:nt tears in sufferers having diagnostic wrist arthroscopy for wrist ache. The incidence of dorsal radiocarpal ligament tears in the presence of other inrercarpal derangements. Frayed ulno-triquetral and ulna-lunate ligaou:nts as an arthroscopic sign of longstanding triquetrq-lunate ligaou:nt rupture. To carry out the check, the patient actively supinates the forearm whereas the examiner makes an attempt to "hook" the distal biceps u:ndon from the lateral side. The solely caveat is that if the examiner feels that the distal biceps tendon is intact, the injury could be extra proximal on the myou:ndinous junction or solely a partial tear at its insertion. It is necessary to make the distinction between the widespread full avulsion from the radial tuberosity and an harm at the myotendinous junction, because the extra proximal accidents are finest treated nonoperatively. The forearm is compelled into extension from a flexed place because the biceps muscle fires � Avascular modifications within the distal tendon and possible impingement within the interosseous house between the tuberosity and the proximal ulna might contribute to rupture. This is especiaUy famous in patients who require repetitive supination, similar to mechanics and plumbers. Pain is usuaUy not a predominant criticism, although some sufferers will expertise fatigue-type pain and cramping within the retracu:d muscle stomach. Patients usuaUy present with ache within the antecubital fossa, especiaUy with resisted flexion and supination. The affected person should proceed to strengthening when full painless vary of motion is obtained. Patients must be endorsed that ache is extra of a predominant criticism with these partial accidents. Some authors have said that higher than eight weeks is continual and that a graft is n~ed in these situations. Semitendinosus (either autograft or allograft),sixteen Achilles tendon allograft13 (with the bone plug inserted into the radial tuberosity or simply gentle tissue repair), tlexor carpi radialis autograft,9 and fascia lata6 have been described. Positioning � the patient is positioned in the supine place on an armboard with a sterile tourniquet on the upper arm. Therefore, single-incision anterior approaches have been developed with various strategies of. The lateral antebrachial cutaneous nerve and superficial radial nerve are recognized and protected. The goal is to create a locking sew proximally and allow about 1 em of the distal biceps tendon to be unlocked. One of the passing sutures is independently pulled, drawing the tendon into the radial tuberosity. We use fluoroscopy to affirm placement of the button� the passing sutures are then pulled fully out after anatomic tendon placement is visually confirmed. In the case of interference screw fixation, a gap is drilled within the radial tuberosity. The diameter ofthe gap � is decided by the system (and the dimensions of the screw) getting used. Some authors use two suture anchors, and most use some type of a sliding knot to advance the tendon onto the bone. A second longitudinal incision is made 1 em radial to the subcutaneous border of the radius within the proximal forearm on the stage of the biceps tuberosity. Dissection is initially made in the extensor carpi ulnaris muscle and then by way of the supinator musde. Take nice care to keep away from subperiosteal dissection on the ulna to lower the risk of synostosis. The sutures are then handed via the drill holes and tied over bone with the forearm in supination. This may be completed by creating a second incision on the medial facet of the distal arm. A more meticulous dissection is required to defend the lateral antebrachial cutaneous and musculocutaneous nerves.
References
- Kraus JP, Williamson CL, Firgaira FA, et al. Cloning and screening with nanogram amounts of immunopurified mRNAs: cDNA cloning and chromosomal mapping of cystathionine beta-synthase and the beta subunit of propionyl-CoA carboxylase. Proc Natl Acad Sci USA 1986;83:2047.
- Ren J, Kaplan P, Charette M, et al. Time window of intracisternal osteogenic protein-1 in enhancing functional recovery after stroke. Neuropharmacology 2000;39(5):860-5.
- Armstrong DG, Lavery LA, Harkless LB. Validation of a diabetic wound classifi cation system. The contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care. 1998;21:855-859.
- Baker BM, Lindsay BD, Bromberg BI, et al. Catheter ablation of clinical intraatrial reentrant tachycardias resulting from previous atrial surgery: localizing and transecting the critical isthmus. J Am Coll Cardiol 1996;28(2):411-417.
- Blumberg HM, Jarvis WR, Soucie M, et al. Risk factors for candidal bloodstream infections in Surgical intensive care unit patients: the NEMIS prospective multicenter study. Clin Infect Dis. 2001;33(2):177-186.