

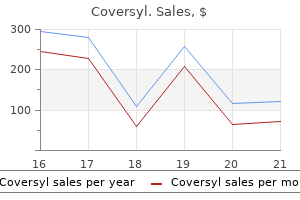
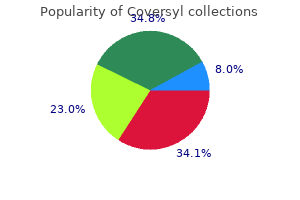
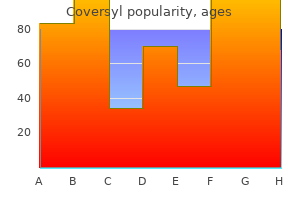
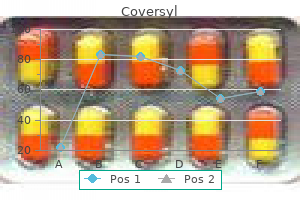
Coversyl
Claire Bouvattier, MD
- MCU, Paris Descartes University
- PH,
- Cochin-Saint Vincent de Paul, Paris, France
Coversyl dosages: 8 mg, 4 mg
Coversyl packs: 10 pills, 30 pills, 60 pills, 90 pills

Coversyl 8 mg amex
The most typical is stricture formation medicine zocor coversyl 8mg free shipping, which frequently requires serial endoscopic dilation or surgical resection medications names and uses 4 mg coversyl mastercard. A historical past of caustic ingestion predisposes the patient to a much larger risk of esophageal squamous cell carcinoma all through life as well medicine names generic coversyl 4 mg without prescription. The commonest cause of higher gastrointestinal bleeding is ulcerative disease of the stomach or duodenum. Esophageal causes of hemorrhage embody varices, Mallory-Weiss tear, esophagitis, and neoplasms. Esophageal varices are mostly associated with portal hypertension on account of cirrhosis of the liver. On endoscopy, these varices usually appear as tortuous blue or white submucosal lesions. Endoscopic sclerotherapy or clipping or systemic medicine, such as vasopressin or somatostatin, are frequently used for acute variceal bleeding though uncontrolled life-threatening bleeds could require balloon tamponade. Asymptomatic varices seen upon endoscopy are a severe finding since such sufferers often present with life threatening hematemesis that may be avoided with beta-blockers or surgical shunts. Treatment options for life-threatening energetic bleeding embrace endoscopic clipping, electrocautery, or injection of saline with epinephrine. Dysphagia is the most common symptom that ensues and relies on the scale and location of the mass. These are usually discovered within the distal esophagus, where clean muscle predominates. These neoplasms usually occur as a single mass and may be tough to visualize on endoscopy. Enucleation at thoracotomy is an effective remedy for large symptomatic leiomyomas. Acute inflammation could result in progress and the subsequent development of symptoms. On esophagoscopy, the cyst could appear as a blue, clean, round mass beneath an intact layer of mucosa. Fibrovascular polyps are intraluminal lesions which are discovered within the higher esophagus or the postcricoid region. Laryngeal obstruction with subsequent asphyxiation by a regurgitated fibrovascular polyp is a well-described cause of death. There is often a big vessel in the stalk of the polyp that should be addressed during resection. While fluoroscopy may counsel the presence of malignant neoplasms, essentially the most sensitive method of detecting esophageal cancer is endoscopy with biopsy. Most signs of esophageal carcinoma are nonspecific and include weight loss, vomiting, and gentle hematemesis. With uncommon exception, all sufferers with solid meals dysphagia ought to be evaluated for esophageal carcinoma by esophagoscopy. More than half of patients with esophageal malignancies have distant metastases on the time of prognosis. Squamous cell carcinoma of the esophagus has been historically thought of the commonest malignancy of the esophagus, however this is changing. Among cancers, the incidence of adenocarcinoma of the esophagus is the fastest growing in America and is now greater than its squamous cell counterpart. On esophagoscopy, adenocarcinoma might seem as a mucosa-covered nodule or as an ulcerative mass with esophageal obstruction in more advanced instances. As talked about earlier, esophageal malignancies could spread throughout the size of the esophagus from any main web site because of the intensive, interconnected lymphatic community. Therefore, the entire esophagus is often handled regardless of the main location in the esophagus. Primary surgical therapy, often with total esophagectomy and gastric pull-up or colonic interposition, is the standard mainstay of esophageal carcinoma treatment, with chemotherapy and radiotherapy used for lesions that invade the muscularis or deeper. In the presence of distant metastases, palliation with esophageal stents is often the only therapy supplied. Paper presented at: 87th Annual Meeting of the American Broncho-Esophageal Association; April 26�27, 2007. Wireless pH testing as an adjunct to unsedated transnasal esophagoscopy: the security and efficacy of transnasal telemetry capsule placement. Unsedated transnasal esophagogastroduodenoscopy for the analysis of dysphagia following treatment for previous major head [sic] neck most cancers. Prediction of simultaneous esophageal lesions in head and neck squamous cell carcinoma. Detection of metachronous esophageal squamous carcinoma in sufferers with head and neck cancer with use of transnasal esophagoscopy. Functional oesophagoscopy: endoscopic evaluation of the oesophageal phase of deglutition. Patient tolerance of in-office pulsed dye laser remedies to the higher aerodigestive tract. Perforation after inflexible pharyngo-oesophagoscopy: when do signs and indicators develop Eroglu A, Turkyilmaz A, Aydin Y, et al Current management of esophageal perforation: 20 years expertise. Esophageal perforation in adults: aggressive, conservative remedy lowers morbidity and mortality. Prevalence of penetration and aspiration on videofluoroscopy in normal people with out dysphagia. Eosinophilic esophagitis: medical features, endoscopic findings and response to remedy. Eosinophilic esophagitis in youngsters and adults: a systematic review of sufferers with dysphagia attributable to benign problems of the distal esophagus. Eosinophilic esophagitis in adults: an rising downside with unique esophageal options. Endoscopic evaluation of esophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Chicago classification standards of esophageal motility disorders outlined in high resolution esophageal stress topography. Esophageal motility disorders when it comes to pressure topography: the Chicago Classification. Bethanechol improves clean muscle perform in patients with extreme ineffective esophageal motility. Esophageal motility issues (distal esophageal spasm, nutcracker esophagus, and hypertensive lower esophageal sphincter): trendy administration. Use of botulinium toxin for prognosis and administration of cricopharyngeal achalasia. Flexible versus rigid endoscopy for treatment of foreign physique impaction in the esophagus.
Order coversyl 4mg without prescription
Anteroposterior (A-P) Supraglottal Compression Koufman and Blalock have introduced a voice kind labeled "Bogart-Bacall Syndrome" treatment kawasaki disease generic 8mg coversyl fast delivery, in which patients exhibit a tension-fatigue dysphonia with phonation on the backside of their vocal dynamic ranges treatment jock itch buy generic coversyl 4mg online. Hypertonicity in the thyrohyoid muscles is typically famous along side the A-P constriction medicine vs nursing cheap coversyl 4mg on-line. Singers may exhibit an identical A-P contraction pattern on phonation in affiliation with tense pharyngolaryngeal postures. This sample may be used to achieve a selected resonance high quality, an instance or which is native North American throat singing, but in different singers it could be unintentional and secondary to technical error. Transnasal fiberoptic examination throughout related speech or singing is the simplest method to demonstrate this misuse. Elicitation of slow glissando pitch glides could impact some release of the A-P constriction. Incomplete Adduction in Conversion Reaction Dysphonia the emotional stressor or conflict that leads to a conversion response has produced such psychological distress that a bodily symptom similar to aphonia is extra bearable to the person. Forced adduction, distraction, glottal fry or excessive pitches could elicit vocal fold approximation throughout diagnostic remedy, in which case the profitable approach is used to initiate remedy in the absence of unresolved psychological gain factors that will have an effect on motivation to obtain regular voice. Bowed Vocal Folds Associated with Psychogenic Dysphonia In older patients, presbyphonia is related to lack of muscle bulk and tone, in addition to weakening and fragmentation of elastin and collagen fibers. Occasionally, sufferers who seem to have a psychogenic dysphonia will phonate with a bowed glottis but could resume normal phonation and laryngoscopic look after voice therapy, psychotherapy, or both. This also could characterize one of the forms of dysphonia in "habituated hoarseness" that follows an upper respiratory tract an infection or other natural trigger. Falsetto Register in Adolescent Transitional Voice Disorder Normal adolescent voice change throughout puberty usually is accompanied by pitch breaks, register breaks, and self-consiousness about speaking. Emotional factors could lead to inhibition of the transitional event and institution of perpetual falsetto phonation. The larynx typically is elevated by suprahyoid muscle contraction so it approximates the hyoid bone or base of tongue. During the fibreoptic laryngeal examination, extra applicable phonation may be elicited with a cough/throat clear; glottal fry register; effort closure; loud phonation; or coordinated voice onset ("Hm! It seems that there are 2 primary altered states in the larynx that develop with getting older. One, which predominates in women, is a thickened, chronically edematous larynx, leading to a naturally lower f0 that might be under the typical "genderambiguous" f0 round 160 Hz, generally with accompanying dysphonic options. These sufferers, most of them males, develop the next f0 which can be above the gender-ambiguous f0, and thin voice timbre. Other age-related adjustments � similar to lowered important capability, reduced elasticity in structures of the chest wall, and lowered strength in articulators � can all contribute to altered speech and voice dynamics and muscle misuse patterns. Detailed information about neurogenic issues of the larynx is provided in Chapter ninety one. Medical and surgical procedures used to deal with disorders widespread to the aged, such as cardiovascular disease, might lead to peripheral nerve harm, mostly to the left recurrent laryngeal nerve disturbed throughout cardiac surgical procedure or intubation accidents in the larynx during basic anesthetic. Hearing loss may play a job in voice changes as self-monitoring becomes tougher. Finally, in older patients, loneliness or separation from family, lack of independence, and different life-style adjustments might result in adjustment problems with despair and anxiety, which may contribute to muscle misuse affecting the larynx. The growing older process within the male larynx includes muscle atrophy and loss of elasticity. Attempts to compensate for these changes often lead to glottal fry phonation, elevated laryngeal effort, and fast vocal fatigue. Indirect laryngoscopy reveals obvious shortening and bowing of the true vocal folds. The vocal folds could adduct extra effectively if lengthening can be achieved by larger pitched voice. Those women who try and correct the pitch change by compensatory muscle misuse could develop lateral glottal and supraglottal compression and elevated vocal effort. This tactic may fit to a degree, however quickly the dysphonic voice resulting from muscle misuses related to the attempted compensations are a larger problem than the pure adjustments causing the low pitch. Similarly, the old man with an simply tiring "glottal fry" phonation and bowed vocal folds could additionally be suffering more from his unconscious try and drive the vocal pitch all the way down to the male range than from the muscle atrophy, fragmented collagen, and weakened elastin of his larynx. The laryngospasm may produce airway obstruction, more typically inspiratory than expiratory, and this is usually referred to as "vocal wire dysfunction" or "paradoxical vocal cord movement". It might result in voice difficulties, manifest as episodes of tight, strained, spasmodic voice. The overreaction to regular sensory stimuli may be publish viral, or related to neuroplastic modifications within the central nervous system subsequent to repetitive noxious stimuli impacting muscle reactivity within the larynx and related buildings of the embryologically-related neuromuscular methods of respiration and swallowing. Classifications presented by the World Health Organization have supplied theoretical foundations for these tools. Table 93-4 presents current self-report inventories that could be useful for sufferers and clinicians to elucidate the overall influence of voice dysfunction, to provide indications for treatment priorities and to measure therapy outcomes. In some individuals, reflux could also be play a major position in predisposing, precipitating and/or perpetuating the hypertonicity, and an acceptable degree of reflux management is designed as a priority. In different circumstances, reflux might not seem to contribute considerably to muscle misuse patterns, and focus for administration may be primarily on altering specific features of life-style, method and/or approaches to coping with emotions and personality characteristics. Voice Therapy Voice remedy packages are best managed by speech-language pathologists with experience in disorders of the larynx. Indirect therapy is usually supplied to decrease way of life components contributing to muscle misuse. This includes affected person training, and insight and modification of any related behavioural, ergonomic and environmental elements which would possibly be contributing to muscle misuse. Suggestions may be made about modifying workplace ergonomics and acoustic characteristics, utilizing voice amplification methods, and/or altering people administration kinds, for example, utilizing non-vocal approaches to behavioral administration in the classroom. This entails presentation, demonstration, instruction, and typically handbook facilitation of methods which are recognized to positively impression the particular muscle misuses identified. In cases where muscle misuse in the larynx is associated with basic physique posture misuses, voice rehabilitation will include a complete hierarchical motor re-learning program for body alignment, acceptable use of muscle tissue around the head, neck and shoulders, specific adjustments and workout routines for tongue, jaw and facial muscles. If dysphonia is associated with the muscle misuse drawback, motor re-learning activities will be launched to enhance speech respiration and voice onset, resonance, vocal flexibility, vocal dynamics and significant speech phrasing. This sort of complete program is commonly offered in a gaggle format, which might offer time and monetary efficiencies to numerous individuals needing similar instruction and mutual help. Self-evaluation inventories are used at numerous stages to help clinician and affected person chart progress and document areas that need more intense focus. A self-help guidebook is utilized in our clinic to present specific path for apply. Focused direct therapy may be used to take care of short-term, specific signs of muscle misuse. Technique(s) are sometimes probed in the course of the voice assessment to decide the best method, then explored additional in direct therapy and shaped into extra appropriate muscle perform for speech, or leisure or the laryngeal valve system. For example, a 15-year-old boy with adolescent transitional voice disorder sometimes makes use of the posture for falsetto throughout speech. By manually releasing the larynx down and/or initiating a cough or glottal fry, modal register could additionally be produced.
Trusted 8 mg coversyl
Activation of p53 gene expression in premalignant lesions throughout head and neck tumorigenesis medications erectile dysfunction 4mg coversyl sale. Immunohistochemical detection of p53 protein accumulation in head and neck cancer: correlation with p53 gene alterations medicine 801 trusted coversyl 8mg. Biomarkers Predict p53 Gene Therapy Efficacy in Recurrent Squamous Cell Carcinoma of the Head and Neck medications 126 cheap 4mg coversyl mastercard. An adenovirus mutant that replicates selectively in p53-deficient human tumor cells. Oxygenation of squamous cell carcinoma of the top and neck: comparison of main tumors, neck node metastases, and regular tissue. Phase I trial of concurrent tirapazamine, cisplatin, and radiotherapy in patients with advanced head and neck cancer. Development of a hypoxia gene expression classifier with predictive influence for hypoxic modification of radiotherapy in head and neck cancer. A 26-gene hypoxia signature predicts benefit from hypoxia-modifying therapy in laryngeal cancer but not bladder cancer. New users of metformin are at low risk of incident most cancers: a cohort research amongst people with type 2 diabetes. Early-stage disease at many sites has frequently been treated efficiently with radiotherapy alone. Historically, extra superior cancers have been addressed by surgery as the primary modality with postoperative radiation therapy when indicated. However, large strides have been made within the realm of mixed radiotherapy and chemotherapy such that organ preservation is now the rule quite than the exception in many head and neck sites. In cases during which surgery is indicated, advances have also been made in the supply of postoperative mixed modality therapy. In truth, inside months of the invention of the "New Light," at least one visionary had already carried out palliative "roentgentherapy" on a patient with recurrent-breast cancer. The introduction of megavoltage radiotherapy delivered via a linear accelerator, or "linac," marked the dawn of the fashionable radiation era. The capacity to generate high-energy photons enabled practitioners to deal with not solely superficial lesions successfully but additionally deep-seated tumors. Improvements in patient immobilization with using thermoplastic masks and other related devices have allowed for reduction in unsure margins and enabled better general treatment accuracy. Inverse planning refers to the method by which an idealized radiation dose distribution is first outlined, and an iterative pc algorithm is subsequently employed to achieve optimally that distribution. In a similar method discount of radiation dose publicity to the pharyngeal constrictors and larynx can decrease the dysphagia rates. Traditionally it can be used as a definitive therapy modality for T1-T2 lesions, postoperatively or as a boost to bigger lesions initially treated with external-beam radiation. This contains session with the next: 1) dentistry to provide fluoride trays and different prophylaxis for serviceable teeth or extraction of poor dentition Many Radiation Oncology Departments together with ours routinely suggest usage of dental guards designed to defend mucosal surfaces positioned by steel crowns or fillings from backscatter radiation. Individually designed lead defend encased in a plastic safety can be utilized when brachytherapy of the lips, the cell tongue, the oral mucosa, or the floor of mouth is deliberate near the mandible, to reduce the dose to the mandible and to avoid osteoradionecrosis; 2) diet to educate the patient and institute measures to minimize weight reduction and deconditioning during treatment; and 3) speech remedy in anticipation of future points with speech and swallowing. Primary endocrinologic evaluation can additionally be prudent in view of the potential thyroid or pituitary dysfunction related to treatment of certain head and neck sites. Images through the anatomic space of curiosity are then obtained at three to 5 mm intervals. Reference marks are made on the thermoplastic mask to reproduce day-to-day patient setup. The doctor "contours" these volumes, and radiation fields are then positioned by trained dosimetrists, under the guidance of the radiation oncologist, to embody the contoured volumes. Due to the low threshold for potential damage to the spinal cord, doses above approximately 45 to 50 Gray (Gy) to that organ are thought of unacceptable. Therefore, "off wire" lateral fields by which the posterior border of the sphere lies anterior to the spinal wire, for instance, at the midvertebral body within the sagittal plane, are initiated prior to reaching the tolerance dose. To treat probably involved lymph nodes mendacity in the region posterior to the "off cord" fields adequately, electron fields ("posterior-electron strips") are utilized. Electron therapy deposits dose superficially compared to photons, with speedy dose fall-off at depth. The lymph nodes of curiosity are positioned comparatively near the floor and receive the prescribed dose, however the spinal wire, a deep structure within the sagittal aircraft, is actually spared. Finally, a 3-D "increase" subject is designed to encompass only areas of gross tumor and a margin to account for setup uncertainty and inner anatomic motion. The delivery of definitive doses of radiation has, at instances, been restricted by the danger of normal tissue damage. Given the anatomic proximity of important structures, tumors of the head and neck current a significant therapeutic challenge. Standard-beam arrangements and treatment-planning strategies are able to achieve uniform-dose supply throughout the complete anatomic area. The capability to deliver a homogeneous dose to a tumor-bearing region is fascinating; however, it proves to be an obstacle when it comes to dose delivered to surrounding crucial structures. A clear rationale exists for this marriage of modalities in that chemotherapy and radiotherapy can mix in an additive, and even supra-additive trend to enhance tumor kill by multiple mechanisms. In general, the aim of including concurrent chemotherapy to radiation is to improve the therapeutic ratio. Therefore, at a given degree of normal-tissue harm, a higher chance of tumor control is achievable. Various strategies are available to measure the consequences of chemotherapy and radiotherapy either in vivo or in vitro. In vitro strategies entail subjecting cells in culture to numerous therapies to assess response. The possible interactions of combined chemotherapy and radiation have been promulgated by Steel in a traditional paper. Note that the improvement in tumor management when drug is added exceeds the rise in normal-tissue harm; ie, the therapeutic ratio is improved. G1 G2 S independence, referring to the concentrating on of various anatomic sites by the respective modalities without overlapping toxicity. Decades of subsequent analysis have helped elucidate the interaction of chemotherapy and radiation, although much stays incompletely understood. Taxanes have confirmed to be potent radiosensitizers with resultant use in treating cancers of varied sites, including the head and neck, esophagus, lung, breast, bladder, pancreas, and female urogenital techniques. The success of taxanes in combination with radiotherapy highlights the influence of the cell cycle on radiation sensitivity, as first described by Terasima and Tolmach almost half a century in the past. Therefore, any agent that promotes the accumulation of cells within the sensitive phase of the cell cycle and/or selectively eradicates cells within the resistant part will optimally mix with radiotherapy. Taxanes, which bind to b-tubulin and thereby increase polymerization to promote stable-microtubule era, arrest cells within the radiosensitive G2/M phases. The trial included quality of life research and useful assessments concerning communication, swallowing, and consuming. At six, 12, and 24 months, the patients with a preserved larynx reported higher communication scores, although there was no statistical distinction in swallowing operate.
Generic 8mg coversyl fast delivery
The three common methods that may be employed are (1) concomitant single-agent or mixture chemotherapy with continuous-course radiation; (2) combination chemotherapy with deliberate split-course radiation; and (3) rapidly alternating chemotherapy and radiation medications you cant take while breastfeeding order coversyl 4mg online. More just lately treatment yeast infection home remedies cheap coversyl 8mg line, altered-fractionation radiation approaches have turn out to be a further radiotherapy choice medicine 8 pill order coversyl 8mg fast delivery. Currently, one of the best proof helps concurrent chemoradiotherapy with a platinum-based agent as the standard of care for domestically advanced head and neck most cancers, however recommendations may change as new data turn into obtainable. Concurrent Chemoradiation the first examine to investigate concomitant chemoradiotherapy for the treatment of unresectable advanced head and neck cancer was reported in 1992 (7 5). Surgical resection was offered for sufferers in all three teams if feasible after the completion of therapy; sufferers in the third arm had an choice for surgical resection after the second cycle of chemotherapy, if feasible (76). This study demonstrated a major survival advantage at 3 years for sufferers treated with concurrent cisplatin and radiation (37%) compared with radiation alone (23%; P = 0. The split-course concurrent regimen provided no survival advantage (27%) over radiation alone. Grade 3 toxicity or higher was significantly extra frequent with concurrent remedy (89%) compared with radiation alone (52%; P < zero. This study established radiation with concurrent high-dose dsplatin as the standard of take care of domestically advanced unresectable head and neck most cancers. A meta-analysis of randomized concurrent chemoradiotherapy research for patients with locally superior squamous cell cancer of the top and neck was carried out to develop medical suggestions (79). The meta-analysis advised that platinum-based regimens for concurrent chemoradiation that were related to a constructive trial and a extra favorable side-effect profile ought to be used. Overall, cisplatin-based chemoradiotherapy offered the most significant benefit by method of survival and localregional control (80). The information showing improvement are best established for platinum-based concurrent regimens; a bonus for the use of chemotherapy persists even when newer altered-fractionation radiotherapy approaches are employed. The response fee to Chapter 111: Cnemoradiation 1701 induction with the three-drug routine was significantly larger compared with that of the two-drug regimen (68% vs. Less toxicity was obseiVed with the three-drug mixture than with the two-drug mixture. Definitive local therapy in each arms consisted of ordinary radiotherapy plus weekly carboplatin. Chemoradiation was planned following induction chemotherapy but the precise treatment was not uniform. The results of those trials may redefine the standard of take care of unresectable disease. The experimental arms ofboth research consisted of ordinary fractionation radiation with concurrent cisplatin on days 1, 22, and 43. In each studies, concurrent chemoradiotherapy was related to higher toxicity. While the experimental treatment arms have been comparable for both research, the definition of high-risk pathologic options differed between research. In an attempt to reconcile the differing results of these two trials, a pooled evaluation was carried out which confirmed that the subset of patients in both trials who received a big benefit from the addition of cisplatin to postoperative radiotherapy had either microscopically involved margins or extracapsular extension of illness in neck nodes (86). The presence of either or each of these threat factoiS is therefore now considered a particular indication for adjuvant chemoradiation. In preclinical research, cetuximab demonstrated a minimal of additive results when combined with radiotherapy or with cisplatin, paclitaxel, and different cytotoxics. This trial randomly assigned patients with locally advanced squamous cell cancers of the oropharynx. The addition of cetuximab considerably improved local-regional failure-free survival and total suiVival charges: median local-regional failure-free suiVival was 24. Cetuximab is associated with the development of an acneiform rash in 84% of patients throughout remedy, which is prominent in 73% of sufferers. Of the patients who acquired cetuximab, those that developed a distinguished cetuximab-induced acneiform rash had longer total suiVival (69 months) in comparability with these with gentle rash (26 months), which was significant (P = zero. A limitation to this research is extrapolation of the outcomes to the bigger head and neck cancer inhabitants: cetuximab was only studied in combination with radiotherapy, using radiation alone because the management group. In addition, the examine population was heterogeneous with respect to resectability, primary site, and radiation schedule. Whether the mixture of radiotherapy and cetuximab is as efficient as the standard of chemoradiation is unknown. At the present time, the one indication for cetuximab with radiotherapy is in the treatment of sufferers whose age, efficiency status, or comorbidity precludes remedy with platinumbased chemoradiation. Cetuximab with radiotherapy supplies a 9% absolute survival advantage at 5 years over radiotherapy alone. Numerous trials are at present testing the addition of cetuximab or small-molecule tyrosine kinase inhibitors to chemoradiation in numerous illness settings. Less generally used drugs that additionally present some exercise against head and neck tumors are bleomycin, irinotecan, gemcitabine, capecitabine, oxaliplatin, cyclophosphamide, ifosfamide, pemetrexed, and biologic brokers similar to cetuximab. Randomized trials comparing mixture chemotherapy and single-agent remedy show an approximate doubling of the response rate with platinum-based combinations of chemotherapy. While quite a few single brokers have activity towards head and neck cancers and can be used, weekly methotrexate is the historical gold normal because of its ease of administration, lower toxicity profile, and relative decrease prices (95). A poor response to palliative chemotherapy may be predicted for sufferers with poor performance status, the presence of comoroidities, cumbersome local-regional disease or high tumor volume, and prior therapy for recurrence. Despite the favorable outcomes of the use of taxanes in induction chemotherapy protocols, no improvement in survival with the utilization of taxanes has been dorumented for sufferers with recurrent illness. A study evaluating two different weekly schedules of paditaxel in patients with rerurrent illness provided no advantage in contrast with weekly single-agent methotrexate (96). In a randomized trial of 123 patients Chapter 111: Cnemoradiation 1703 comparing the combination of dsplatin and placebo with dsplatin and cetuximab, no important distinction was present in median progression-free survival (2. There also is a role for this strategy in the organ-preservation and larynxpreservation setting and for superior local-regional nasopharyngeal most cancers. The data displaying enchancment are best established for platinum-based concurrent regimens; a bonus persists even when newer altered-fractionation approaches are employed. Induction chemotherapy results in superior rates of laryngeal preservation in advanced hypopharyngeal cancer. Adjuvant chemoradiation is indicated for sufferers with high-risk pathologic options of extracapsular spread or constructive margins. The use of biologic therapy with radiation offers a survival profit in patients with superior head and neck most cancers who would in any other case solely be candidates for radiation alone due to contraindications to the use of chemotherapy. Current evidence-based indications for standard of care use of chemoradiation are listed in Table 111. Clinical trials testing the addition of cetuximab to concurrent chemoradiation, and induction chemotherapy with the addition of a taxane are in progress. The results of these trials could redefine the usual of care for both resectable and unresectable illness.
Order coversyl 8mg with visa
These lesions seem white and opaque and end in an hourglass closure sample of the glottis treatment of shingles best 8 mg coversyl. These are most seen at greater registers of phonation as the stretching of the vocal folds thins the density of the fold medications pancreatitis buy coversyl 8mg low price, allowing more obvious pathology treatment centers order coversyl 8 mg line. Nodules will decrease the propagation of the mucosal wave depending on their size and fibrous content. Given the potential for vocal fold scarring, multiple elements should be discussed with the patient prior to undergoing invasive therapy. The main aim of surgical intervention should be to return the larynx to a pre-morbid state, thus restoring regular laryngeal perform. These strategies are referred to as microflap, minimicroflap, or subepithelial resections. In sure circumstances, the benefits of eradicating pathology may not outweigh the dangers of performing microsurgery. Unfortunately, the ideal surgical patient is commonly the patient least more likely to benefit from surgical intervention. Those sufferers embrace people with low vocal demands and accessible pathology (large polyps). The patients that can likely profit the most from intervention (those with excessive vocal demand) are additionally those most-likely affected from any complication of the procedure. It is an extension of the laryngeal ventricle and spans posterolaterally to the edge of the laryngeal floor of the epiglottis. Both laryngoceles and saccular cysts contain expansion of the saccule to kind a mass. Laryngoceles by definition include air within the lumen, while saccular cysts are fluid-filled lots. Laryngoceles include a patent communication with the laryngeal lumen, thus allowing air passage. External laryngoceles are situated entirely exterior of the laryngeal framework and combined laryngoceles comprise both inside and external components. Saccular cysts are also categorised according to their location and are brought on by irregular dilation of the saccule. Traditionally, saccular masses are seen in people who develop excessive intralaryngeal pressures (glass blowers, trumpet players). Superinfection can result in fast growth and acute presentation with worsening signs, fever, and sometimes airway obstruction. Diagnostic Principles Patients with laryngoceles and saccular cysts report a spectrum of dysphonia, dysphagia and even airway obstruction depending on the dimensions and placement of the lesion. The prognosis is mostly made by bodily examination including transnasal or transoral laryngeal imaging and neck examination. In the case of anterior saccular cysts, a mass can be seen emanating from the vestibule to the laryngeal lumen whereas lateral saccular cysts and laryngoceles current as a submucosal mass within the false vocal fold. External and combined laryngoceles can present as a neck mass that enlarges with valsalva. Treatment Principles Although controversy exists in the literature as to the surgical management of laryngoceles and saccular cysts, most authors agree that surgical procedure is the definitive management. Endoscopic treatment of those lesions entails either full resection versus marsupialization. However, with advanced instrumentation, visualization, and surgical technique, laryngofissure is commonly unnecessary. Fluid-filled mass arising from the saccule and protruding into the laryngeal lumen. Axial computed tomography displaying air-filled dilation of the saccule extending through the thyrohyoid membrane into the neck. These are brought on by an exophytic tissue response to acute and chonic inflammatory processes. Mechanical causes include vocal hyperfunction and continual chough, and nonvocal laryngeal trauma as seen in intubation damage. Any supply of inflammation can result in local tissue harm that will then cascade into an analogous exophytic response. Compounding this case is the truth that these sufferers are also likely to develop vocally abusive behaviors corresponding to chronic cough and throat clearing which is able to further the inflammatory response. Globus sensation and throat ache may be localized to the greater cornu of the thyroid cartilage, usually on the ipsilateral facet. A thorough history ought to embrace questions detailing circumstance surrounding the onset of signs, for example, intubation, higher airway an infection, coughing, changing vocal demands. Patients with lesions that current in an atypical location or with an appearance worrisome for malignancy should bear biopsy for diagnosis, notably if the patient has risk components for carcinoma. In the event of failure of outpatient administration, the patient should be referred to a gastroenterologist for further workup, and different sources of ongoing vocal trauma should be investigated. Persistent dysphonia despite maximal medical remedy is also an indication for surgery. Microsurgical resection entails amputation of the granuloma at its base maintaining the integrity of the underlying cartilage. Care ought to be taken operating in the posterior part of the glottis to reduce trauma and stop scarring or harm to the cricoarytenoid joint. Patients may benefit from a short course of post-operative voice relaxation to promote healing. Injection of the laryngeal adductory musculature with botulinum toxin may be of benefit as an adjuvant treatment. Theories for the congenital and acquired pathogenesis of sulcus vocalis have been offered. Vocal-fold scarring is classified in accordance with its underlying etiology: traumatic (blunt, penetrating, radiation, surgical procedure, glottic carcinoma), iatrogenic (vocal wire surgical procedure, extended intubation, tracheostomy), and inflammatory (inhalation injury, rheumatic diseases). Typical complaints are of dysphonia characterised by hoarseness, breathy voice quality, and vocal fatigue. Endoscopic findings for these two entities are additionally related and embrace an uneven spindle-shaped glottic closure sample medial furrows or troughs on the glottic margin, and supraglottic hyperfunction. High-resolution videostroboscopic imaging with careful evaluation is most often necessary to determine these delicate lesions. This examination will show disruption of mucosal wave with focal adynamic segments at the website of the lesion. Treatment Principles Treatment for sulcus vocalis and vocal-fold scarring ought to be directed at bettering glottal efficiency and voice quality. Bilateral, proper bigger than left, postintubation granulomas on the vocal processes. Surgical methods embody medialization thyroplasty, injection thyroplasty, native corticosteroid injection, fat or fascia implantation, and mucosal elevation and redraping.
Syndromes
- Female pattern baldness
- Numbness, tingling, weakness
- Chemicals in the air or in food
- A psychiatrist may also prescribe antidepressants or another medicine to help your sleeping problem and any mood or anxiety disorder you might have.
- For lymphomas, chemotherapy followed by radiation is the treatment of choice.
- Are taking any medicines
Buy 8 mg coversyl amex
The need for inpatient hospitalization is determined by the diploma of airway obstruction symptoms 2 purchase coversyl 4mg amex. Treatment is geared toward reducing laryngeal edema and preventing stasis and crusting of secretions within the airway medications 4h2 cheap coversyl 4 mg with visa. Therapy usually consists of hydration medicine lake discount coversyl 8mg online, humidification of inspired air, and coverings with nebulized racemic epinephrine. Antipyretics, decongestants, and parenteral corticosteroids are sometimes empirically administered to decrease airway inflammation. Artificial airway help (eg, intubation) is critical in a relatively small proportion of sufferers with laryngotracheitis. When needed, nevertheless, intubation should be carried out by skilled personnel, ideally in the operating room, the place maximum airway control can be achieved. Secondary bacterial infection of the airway (membranous croup) might subsequently happen, is extra serious and is often suspected when the patient experiences excessive temperature spikes and exudative, purulent sputum. The microorganisms mostly concerned are Haemophilus influenzae, Staphylococcus aureus, Streptococcus pneumoniae, Moraxella catarrhalis, and hemolytic streptococci. Pediatric viral laryngotracheitis must be distinguished from spasmodic croup, or "false croup," which is a noninfectious form of laryngeal inflammation associated with a gentle, chronic-intermittent, croup-like pattern. Spasmodic croup typically affects kids one to 4 years of age, and the afebrile child generally Table 88-7 Effect of 1 mm of Edema on the Cross-Sectional Area of the Subglottic Larynx in the Neonate, Child, and Adult (Area = r2*) Neonate Child Adult Normal Subglottic diameter (mm) Subglottic radius (mm) Subglottic area (mm2) Effect of 1 mm of edema Subglottic diameter (mm) Subglottic radius (mm) Subglottic area (mm2) Percent discount of airway area *For the sake of simplicity, for these calculations = three. Nocturnal attacks could happen as isolated events or recur over two to three nights, however typically the kid is asymptomatic during the day and the episodes subside spontaneously. Although the cause for spasmodic croup remains unsure, evidence suggests that extraesophageal reflux might frequently be the trigger so applicable testing with 24-hour pH monitoring and antireflux therapy is often indicated. The viral prodrome lasts one to seven days, adopted by the event of a barking cough and sometimes inspiratory stridor. It has been reported that a comparatively giant proportion of adults with this syndrome require airway intervention. Influenza and parainfluenza viruses, rhinoviruses, and adenoviruses are the most typical causative brokers, although many other viruses have been implicated. Such patients current with signs of a generalized viral syndrome (low-grade fever, malaise, rhinitis) and hoarseness with voice breaks, episodic aphonia, and a lowering of pitch. While newer antiviral medications may have some utility in lowering the period and severity when administered within the first 24 hours of clinical an infection, the disease is self-limited and remedy is often centered on supportive care. In the professional vocalist, corticosteroids are sometimes used to reduce the vocal-fold edema, significantly in the course of the restoration section. Herpes simplex an infection is ubiquitous, might have an result on any age group, and, uncommonly, might infect the larynx. Most patients with herpetic laryngitis have been reported in the younger or debilitated. At the time of delivery, a neonate passing by way of the birth canal may contract genital herpes from a mom with active illness. Subsequent herpes an infection within the infant might involve the higher airway; and, if the larynx is concerned, could trigger acute airway obstruction. Adult laryngeal herpes is mostly seen in the immunocompromised patient, though herpetic epiglottic infection causing airway obstruction in otherwise wholesome adults has been reported. Symptomatic remedy is dependent upon the location of involvement; topical or systemic acyclovir or another particular antiherpetic medicine, could hasten restoration. Typical look of the papillomavirus lesionincludes vascular ingrowth (stippling) and a cauliflower-like exophytic floor. Papillomatosis is introduced in higher detail in Chapter seventy seven "Infections and Inflammatory Disorders of the Larynx and Trachea. Children aged two to four years are probably the most incessantly affected group, and sufferers with supraglottis present more frequently in the winter and spring months. The sickness begins rapidly over two to six hours with the onset of fever, sore throat, and inspiratory stridor. As the supraglottic buildings turn into extra edematous, airway obstruction develops. The baby is generally ill-appearing, stridulous, sitting upright, and drooling as a result of swallowing is painful. Lateral delicate tissue radiographs could reveal the traditional "thumb sign" of the edematous epiglottis with a dilated hypopharynx. The baby should be transported to the operating room by the dad and mom, an otorhinolaryngologist, and an anesthesiologist to establish the prognosis and secure an airway. Direct laryngoscopy often will show the epiglottis to be very swollen and cherry pink, as are the aryepiglottic folds and the false vocal folds. The true vocal folds and subglottis sometimes appear to be regular or to be only minimally involved. Treatment is directed at airway upkeep after which towards offering antimicrobial and supportive care. Drawing blood, beginning intravenous traces, obtaining a rectal temperature, or otherwise disturbing the affected person ought to be postponed till the airway is secured. In establishments and not utilizing a highly expert pediatric intensive care staff, a tracheostomy could also be preferable to endotracheal intubation. Transnasal fiberoptic laryngoscopy is the most dependable and mostly employed technique to guarantee decision of the edema before extubation. In adults, supraglottitis is manifest by fever, sore throat, a muffled voice, dysphagia, and odynophagia. The onset of symptoms previous to presentation is often longer than that seen in kids (usually greater than 24 hours). The analysis of supraglottitis is made by observing the swollen, bright-red epiglottis and/or supraglottic constructions with fiberoptic laryngoscopy or a swollen epiglottis and dilated hypopharynx on a lateral neck radiograph. The medical course appears much less extreme, with much less seasonal variation and airway compromise. Conservative measures embrace oxygenation, humidification, hydration, corticosteroids, and intravenous antibiotics. Most cases happen from contact with rabbits or squirrels, but many other wild and domesticated animals have been reported to carry the disease. Transmission to people can even happen by a chunk from a tick or a deer fly, which are the intermediate hosts and insect vectors. In people, the commonest portal of entry is thru the skin or mucous membranes. Oropharyngeal tularemia, which occurs in approximately 1% of patients, produces an intense exudative pharyngitis associated with lymphadenopathy. Glanders At one time in history, glanders was "the plague of horses," and, secondarily, it affected man. Today, glanders is uncommon around the globe but still happens in Asia, Africa, and South America. The illness is attributable to an infection by the bacterial organism Pseudomonas mallei (Burkholderia mallei). Transmission remains to be by contact with an contaminated horse or by inhalation or inoculation of contaminated material, and contaminated people are almost completely horse handlers. Infection by inhalation produces an intense, ulcerative mucopurulent granulomatous reaction in the mucous membranes of the aerodigestive tract and pneumonia.
Discount coversyl 4mg free shipping
Selective neck dissections for squamous carcinoma of the upper aerodigestive tract: patterns of regional failure treatment 4 ringworm discount coversyl 4 mg online. Detection of minimal residual cancer to investigate why oral tumors recur despite seemingly sufficient treatment symptoms 14 days after iui order coversyl 4mg without a prescription. Rapid molecular detection of metastatic head and neck squamous cell carcinoma as an intraoperative adjunct to sentinel lymph node biopsy symptoms 2 days before period buy coversyl 8mg free shipping. Image-guided systems proceed to evolve and will turn out to be even more priceless as real time imaging turns into obtainable. The function of robotic surgery has quickly expanded because the first feasibility examine by Hockstein et al1 in 2005 and, as the technology continues to develop; there will be additional applications inside the realm of otorhinolaryngological surgery. The improvement of surgical simulators allows use of different strategies to develop surgical abilities. This growth has turn into particularly related for surgical trainees being required to achieve operative competency within a lowered period of clinical publicity when compared to previous generations. This article critiques the roles of those varied technologies and their application in otorhinolaryngology head and neck surgical procedure. Their use in endonasal surgical procedure is to assist the surgeon with intraoperative stereotactic anatomic localization through the usage of computerized tracking units. There are 4 obtainable forms of tracking technology; sonic, electromechanical, optical and electromagnetic. Electromechanical technology was employed early within the adaptation course of and it relied on detectors located throughout the joints of an articulated arm, which had to manipulated be during surgery. However, this technique requires preoperative placement of fiducial markers, re-registration with every intraoperative head movement, and a mechanical arm which was cumbersome in endonasal procedures. A software program interface facilitates this capability to localize the instrument inside the image repository. In electromagnetic methods, the spatial localization is derived from an electromagnetic subject together with the surgical field, by which the place of an instrument connected to this electromagnetic help can be determined. The spatial recognition of the instrument is based on computerized mathematical analysis of the geometrical concordance between virtual and real anatomic points. At the beginning of the surgical procedure, a locatable instrument is used to mark the anatomically corresponding actual factors as exactly as potential. Neumann and colleagues reported their expertise using the electromagnetic InstaTrak system in 109 patients, seventy six of whom had undergone earlier surgery. Setup of the InstaTrak system, together with headset placement, draping, calibration, and verification took lower than 5 minutes in all cases. Orbital fats publicity occurred in two sufferers and was the only reported intraoperative complication. Postoperative complications included persistent synechiae in 4 patients and epistaxis in a single patient. These authors concluded that the know-how was useful for all sufferers undergoing revision sinus surgery, sufferers with cranium base defects or paranasal sinus neoplasms, and sufferers present process main surgical procedure with in depth illness. The optical-based image-guidance system makes use of an infrared digital camera to monitor instrument and head position. Several authors have evaluated the utility of this stereotactic system in neurotologic cranium base surgical procedure and in endoscopic sinus surgery. The use of the image-guidance system was estimated to increase operating room time by 15 to half-hour for the first five cases each surgeon performed. There were no intraoperative issues though there have been three sufferers who experienced epistaxis that occurred within one week after the operation. The main reported drawback was increased operating room time (71%), and the main benefit was an elevated stage of confidence throughout surgical procedure (85%). In addition, most surgeons (92%) anticipated continued use on the same or elevated frequency. In addition, when correctly used, it may lengthen the boundaries of protected and efficient sinus surgery, especially in sufferers with distorted landmarks. However, by the completion of the operation, accuracy had deteriorated by an average of 0. Even at this accuracy stage the authors thought each methods had been useful as a end result of, when properly used, image-guidance systems must be used to identify bigger and not to distinguish margins of security at a millimeter degree. Computerguided endoscopic sinus surgery elevated the mean whole operating room time by 17. However, the precise operating time was not prolonged for the explanation that time required to set-up, calibrate, and register the system was carried out earlier than the beginning of the operation. In addition, the time represented a mean; and once operating room personnel grew to become conversant in the system this metric was lowered to lower than 10 minutes. Computer-Guided Endoscopic Sinus Surgery: Indications Endoscopic sinus surgery is a viable possibility for the management of medically refractory sinonasal inflammatory disease, neoplasms, and skull base defects. However, regularly, the anatomy has been distorted by previous surgical procedure or the illness process. Given the shut proximity of important structures together with the intracranial contents and orbit, even minimal intraoperative disorientation may end up in critical complications. They analyzed 192 studies reporting original knowledge from controlled trials, retrospective cohorts and prospective cohorts that had a controlled population. The perioperative morbidity variables included major, minor and total complications while the patient-reported end result measures have been outlined by a validated disease-specific quality-of-life questionnaire. When coupled with existing surgical navigation systems, it can provide real-time surgical updates. In medical training, simulation can supply a secure and realistic surroundings within which trainees can repeatedly practice scientific eventualities and an outlined talent set without subjecting actual patients to any threat. Simulation expertise offers a platform on which efficient and goal analysis of technical skills may be applied without any surgical risks. The improvement of such systems for uniform, metrics based mostly training and assessment is becoming increasingly essential for training in order that surgical residents can obtain the required stage of competence. This demand limits the amount of time that school can commit to the teaching process. Ethical procurement and correct disposal of both of those assets, the constraints in availability and the price involved limit these as longterm options. In addition, they could not symbolize one of the best fashions for lots of forms of human surgical procedure and strategies. The image-guidance findings must be correlated with all available anatomic landmarks. Although the preliminary costs could additionally be bigger, the long-term prices may be lower than these associated with the more conventional training strategies famous above. While conceptually fairly simple, performing endoscopic sinus surgery safely and successfully is kind of difficult and may pose significant threat to surrounding anatomical buildings together with the skull base, orbit and internal carotid artery. These procedures require coordination of the endoscopes with the surgical devices in a (3D) area.

Generic coversyl 8mg without a prescription
Grossly treatment 3rd degree burns coversyl 4mg, verrucous carcinoma appears as a fungating medications used to treat bipolar disorder 8mg coversyl for sale, papillomatous treatment of strep throat order coversyl 4mg free shipping, shaggy, grayish-white neoplasm. The surface of the lesion is densely keratinized with a well-circumscribed deep margin. Despite occasional local destruction, illness is regionally contained in greater than 90% of patients. Mortality related to this tumor is also uncommon and most commonly related to an aplastic transformation. Use of endoscopic surgical procedure allows removing of the tumor with much less morbidity while preserving the power to treat recurrent disease if essential. Five-year survival charges for surgical remedy of laryngeal verrucous carcinoma had been discovered to be 94% versus 66% five-year survival in patients handled with radiation alone. Overall fiveyear survival for laryngeal verrucous carcinomas(regardless of treatment) has been reported to be 86. These embrace: carcinosarcoma, pseudosarcoma, pseudocarcinoma, pseudocarcinosarcoma, pseudosarcomatous carcinoma, spindle cell carcinoma, spindle cell variant of squamous carcinoma, squamous cell carcinoma with pseudosarcoma, pleiomorphic carcinoma, metaplastic carcinoma and polypoid squamous cell carcinoma. These theories embody the following possibilities: the existence of two synchronous tumors, a carcinoma and a sarcoma from nearby sites (collision tumor); the origin of the tumor from an undifferentiated pluripotential cell which differentiates toward both squamous epithelium and stroma (carcinosarcoma); the spindle cells could also be a non-neoplastic response of the stroma to the presence of the carcinoma (pseudosarcoma), or the spindle cells may be modified malignant epithelial cells (spindle cell carcinoma). This tumor is significantly more common in males by a ratio of thirteen:1 and develops in the seventh decade of life. Patients (87%) report a history of tobacco use and heavy alcohol consumption (65%). Grossly, the majority of these tumors appear polypoid and barely sessile or ulcerated. Spindle cell (sarcomatoid) carcinoma seems as a biphasic tumor composed of two parts:onewhich is squamous cell carcinoma (invasive or in situ); one other composed of a bland or pleiomorphic spindle cell stroma. When both are clearly present, the sarcomatoid and carcinomatous components generally abut one another with minimal areas of mixing. The sarcomatoid portion can vary in look such that the tumor will imitate malignant fibrous histiocytoma, leiomyosarcoma, fibrosarcoma or fibromatosis. Spindle Cell (Sarcomatoid) Carcinoma: Clinical Presentation and Diagnostic Considerations. Hoarseness is the most typical presenting symptom when spindle cell tumors happen within the larynx. Because of the nature of this tumor, sufferers usually current within one 12 months of symptom onset. Laryngoscopy normally reveals a polypoid, exophytic lesion with partial glottic obstruction. Lesions which have to be thought-about embody fibrosarcoma, malignant fibrous histiocytoma, leiomyosarcoma, rhabdomyosarcoma, malignant peripheral nerve sheath tumor, osteosarcoma and chondrosarcoma, to solely mention a few. In addition to the pathologic features described above, the correct diagnosis is made after considering a number of components which embody age and tumor location. Study of the true incidence and behavior of this tumor is difficult because of frequent misdiagnosis. Tumors occurring in patients with a historical past of radiation therapy appear to be more aggressive. With respect to metastases, these tumors ought to typically be approached with the squamous component in thoughts. That is, regional and distant metastatic potential is present thus requiring neck dissection for all however early tumors. In general phrases, our team favors the usage of combination regimens that incorporate platinum analogs and/ or fluoropyrimidines, when palliative remedy is required. As but, the role of novel brokers, similar to gemcitabine and the taxanes, has not been confirmed. In some situations, repeat biopsy, to outline whether or not a sarcomatoid outgrowth dominates, will refine the choice of chemotherapy. Tumors Derived from Salivary Glands Adenoid Cystic Carcinoma: Biology and Epidemiology. The larynx contains subepithelial minor salivary glands which can often lead to the development of sialogenic neoplasms. Adenoid cystic carcinoma is the commonest malignant tumor of the minor salivary glands and there are approximately 120 circumstances of laryngeal adenoid cystic carcinoma reported in the literature. The etiology of minor salivary gland tumors is unclear, however a number of elements have been postulated to play a task. Grossly, the lesions normally seem as exophytic lots with intact mucosal coverage. Batsakis initially outlined 4 histopathological patterns: cribiform, tubular (glandular), stable, and hyaline (cylindromatous). These patterns were refined by the creation of a grading system for adenoid cystic carcinoma. Patients presenting with sialogenic tumors of the larynx mostly present with dysphagia and hoarseness. The duration of symptoms on the time of presentation can vary from two to three months to two to three years. Preoperative willpower of nerve involvement helps to better counsel patients relating to postoperative expectations. The submucosal progress sample usually leads these tumors to present at a later stage. Still, cervical spread has been documented and is extra common in tumors with a stable pattern. Not uncommonly, adenoid cystic carcinoma demonstrates distant metastases to the lungs (most common), bone and liver. With regard to laryngeal lesions, Alavi reported two-year and five-year survival rates of one hundred pc and 75%, respectively. The benefit gained in these patients handled by neutron beam may outweigh the elevated incidence of opposed reactions related to this remedy. The role of the taxanes, gemcitabine, mitomycin C and topoisomerase inhibitors for metastatic adenoid cystic carcinomas has not been outlined. Mucoepidermoid carcinomas are composed of several completely different cell sorts which embrace clear cells, mucoid cells, columnar cells, epidermoid cells and intermediate cells. The classification and grading of the tumor depends on the relative presence of every cell sort. Mucoepidermoid carcinomas have been divided into three totally different grades: low grade, intermediate grade and excessive grade. Low grade mucopidermoid carcinoma is composed of well-formed glandular or cystic spaces lined by a single layer of mucin-producing cells and flattened epidermoid cells. They are more mobile and pleimorphic with larger numbers of intermediate cells and occasional mitoses. Like adenoid cystic illness, laryngeal mucoepidermoid cancers present commonly with dysphagia and hoarseness. Laryngeal mucoepidermoid carcinoma occurs mostly in the supraglottis the place the density of minor salivary glands is highest. Patients with intermediate or high grade mucoepidermoid carcinoma may current with cervical metastases and this ought to be investigated prior to determining treatment.
Buy coversyl 8mg cheap
Suspension direct microlaryngoscopy remains the gold commonplace in opposition to which results from other techniques must be judged symptoms panic attack cheap coversyl 4 mg online. New instruments: a changing view of endoscopic devices and strategies for accurate direct remark of the larynx and per oral laryngeal surgical procedure symptoms 9 dpo coversyl 8mg with amex. Initial experience with a brand new kind of endoscope that has no fiberoptic bundle for imaging medicine 7 generic coversyl 8 mg without prescription. A 585-nanometer pulsed dye laser treatment of laryngeal papillomas: preliminary report. Laser security in otolaryngology-head and neck surgical procedure: anesthetic and educational considerations for laryngeal surgery. Laryngeal examination: a comparison of mirror examination with a rigid lens system. The significance of amassed oropharyngeal secretions and swallowing frequency in predicting aspiration. What have we realized about laryngeal physiology from high-speed digital videoendoscopy Point-touch strategy of botulinum toxin injection for the therapy of spasmodic dysphonia. The tracheobronchial tree comprises crucial anatomical passages by which illness might affect health at any age, infant to aged. Although the importance of those buildings has been acknowledged for lots of of years, bronchology as a self-discipline began nearly one and one-quarter centuries in the past. Advances in treatment have trusted the event of instruments to examine the tracheobronchial tree, ie, bronchoscopes. The utility of bronchoscopy shall be properly demonstrated within the dialogue of airway disorders and their management. The common anterior-posterior diameter is thirteen mm and the transverse diameter is 18 mm. The anterior and lateral walls are formed by roughly 18 incomplete C �shaped rings of cartilage, and the posterior/membranous wall is the trachealis muscle. Approximately one-third of the trachea is within the neck and two-thirds are in the mediastinum. The airway is lined by respiratory epithelium containing a prominent basement membrane and quite a few goblet cells. The length and position of the trachea vary with changes in position of the pinnacle and neck. The trachea is midline in the neck and deviates slightly to the proper at the level of the aortic arch which compresses the left lateral wall. The proper higher lobe bronchus branches into apical, posterior, and anterior segments. After the upper lobe takeoff, the best bronchus continues because the bronchus intermedius. The anteromedial facet of this bronchus gives origin to the right middle lobe bronchus which contains medial and lateral segments. The typical configuration is the superior section adopted by the medial, anterior, lateral, and posterior basal segments. The left bronchus bifurcates from the trachea at 45 deg, a sharper angle than the best bronchus. The higher lobe bronchus offers off the lingula (superior and inferior segment) and continues as the higher lobe bronchus (typically the left higher lobe consists of an apical-posterior and an anterior segment). The left lower lobe bronchus divides into the superior segment followed by the anteromedial, lateral, and posterior basal segments. When doing interventional procedures such as laser and mechanical resection, one can be within millimeters of enormous and if injured probably lethal vascular constructions. The posterior facet of the trachea and the esophagus are separated by the "get together wall. The superior vena cava and azygous vein lay adjoining to the proper anterolateral wall of the distal trachea. On the right, the pulmonary artery lays instantly anterior to the proper and proper upper lobe bronchi. The left and lerft higher lobe bronchi are in shut association with the aorta and the pulmonary artery. Lymph nodes are carefully associated to the trachea, carina, right and left bronchi, and airways within the hila. Medial or Upper lobe Superior rio Anterior Anterior Posterior Up p er d ion Apical- B. In contrast, compression of the lumen initially of a cough contributes to the increased driving strain and increased airflow velocity that promote mucus expulsion; the abrupt noise of the cough outcomes from all of a sudden elevated airflow turbulence. Normal airflow within the trachea is laminar; masses or stenoses obstructing the lumen cause turbulent airflow evidenced as stridor. Their causes may be congenital, infectious, inflammatory, neoplastic, and traumatic. Congenital anomalies that affect the larynx are coated in Chapter seventy five, "Congenital Anomalies of the Larynx and Trachea. In the tracheobronchial tree, congenital stenosis that narrows and obstructs the airway occurs in varied forms. More severe forms embrace segmental stenosis, funnel-shaped tracheal U rd r pe rio Up os the Left primary bronchus Rt. Long-segment tracheal stenosis may be accompanied by an aberrant left pulmonary artery, also known as pulmonary artery sling. Tracheostomy is commonly not helpful for obstructing lesions within the middle or distal trachea. The finest therapy choices for congenital tracheal stenosis include tracheoplastic restore via median sternotomy. The slide tracheoplasty method is at present the procedure of selection for lesions judged favorable for restore. These embody double aortic arch, right aortic arch with left dd Mi l le Superior st. These develop from abnormalities in formation of the major vessels throughout embryogenesis. With progress, often by three years of age, it moves away from the trachea to the best. Pulsatile anterior tracheal compression narrows the trachea lumen in the shape of a tear drop. The lesions are repaired by cardiothoracic surgical procedure, with the potential for cardiac bypass a necessity. Tracheomalacia or bronchomalacia refers to narrowing of the trachea or bronchi with out extrinsic compression or inside stenosis.

Cheap coversyl 4 mg free shipping
These symptoms can range from refined vocal fatigue symptoms 8 days after iui cheap 8mg coversyl with visa, most pronounced when speaking at excessive depth or over background noise to apparent symptoms jaw pain and headache purchase 8 mg coversyl, near-total aphonia medicine reviews order coversyl 4 mg with amex. Patients with unilateral laryngeal paralysis may also report dysphagia, additionally due to glottic insufficiency, although much less typically than voice complaints. Dysphagia-related complaints are extra frequent in sufferers with "high" vagal damage, affecting both superior and recurrent laryngeal nerves, which provides hemilaryngeal anesthesia, pyriform sinus atony and cricopharyngeal muscle hyperfunction to glottic insufficiency from the immobile vocal fold. Situations by which laryngeal anesthesia exists alongside other cranial nerve deficits, as in jugular-foramen syndromes, after stroke or cranium base surgery also carry increased danger of dysphagia. Operations which have an result on pulmonary reserve, as do most thoracic procedures, appear to carry a better danger of aspiration, and age may be an impartial risk issue. More subtle signs include laryngospasm ensuing from reaction to sudden penetration or aspiration. This laryngospasm may happen in patients with surprisingly small levels of glottic insufficiency and fairly good voice quality. Occasionally, sufferers could complain of shortness of breath, particularly during phonation or physical activity. An air-flow loop will inevitably reveal an extra-thoracic obstruction; this obvious discovering, plus a scarcity of insight into laryngeal physiology, might lead the doctor instantly away from measures to medialize the vocal fold, restore glottic perform and relieve these symptoms. When the onset of signs instantly follows an operation which locations laryngeal nerves in danger, no additional seek for cause is important. In other patients, the otorhinolaryngologist should inquire regarding smoking history, the most recent chest imaging, and antecedent illness. Relevant elements embody neurologic signs like weak spot, tremor and dysarthria; pulmonary signs suggestive of tuberculosis or malignancy; and exposure to neurotoxic brokers like stable tumor chemotherapy (vincristine, vinblastine and cisplatin) and organophosphates present in pesticides. The examination of a patient with laryngeal paralysis ought to include careful palpation of the neck for lymphadenopathy or thyroid enlargement. The remaining cranial nerves must be systematically evaluated, with special consideration to the spinal accent and hypoglossal nerves, which share the jugular foramen with the vagus. The presence of ipsilateral tongue deviation, palate droop or Horner syndrome should increase the suspicion of a base of cranium lesion. Flexible transnasal laryngoscopy most likely offers a more correct impression of laryngeal perform than rigid methods, because the tongue traction needed for the latter most likely introduces some artificial biomechanical factors which can be misleading. A hypomobile vocal fold might sometimes be surprisingly tough to recognize; in such patients, asking the patient to alternate sustained vowel phonation and sniffing (the so-called "eeesniff" maneuver) should deliver any asymmetry into stark proof. The examiner ought to take care to not be mislead by small amounts of vocal fold movement which can be brought on by the interarytenoid muscle, nonetheless partially innervated from the contralateral nerve, by an intact cricothyroid muscle, and even by passive lateral displacement of the arytenoid cartilage with its muscular tissues denervated by its pair throughout adduction. We have seen that the place of the paralyzed vocal fold carries no significance with respect to the positioning of the harm or prognosis. Nevertheless, cautious examination can reveal features which can inform medical care. Such three dimensional judgments are tough to make on laryngoscopy, but top mismatch is necessary to identify, as easy medial displacement of the paralyzed fold may not suffice for good apposition throughout phonation. The presence of a prolapsed arytenoid does however suggest profound denervation with lack of muscular assist for the cartilage. In addition, it strongly suggests a top and rigidity mismatch between the vocal folds. These are all components which argue for an arytenoid stabilization process, mentioned further below, ought to surgical rehabilitation be contemplated. Experimental examine has proven the cricoarytenoid joint to be strikingly strong and immune to disruption. The presence of arytenoid edema and erythema, and the absence of a jostle signal are suggestive of cricoarytenoid joint damage and should prompt further investigation, in which electromyography may be of particular utility. In hemilaryngeal paralysis, the glottal hole could also be of two principal configurations. The presence of a posterior gap ought to trigger the otorhinolaryngologist to contemplate an arytenoid stabilization process for rehabilitation as a result of implant medialization alone, or injection augmentation for that matter, is notoriously poor at correcting this deficit. These are necessary to perceive, even if for no other purpose than to help in interpretation of the copious literature in this space. The s/z ratio compares the maximum phonation time of a voiced (/z/) and voiceless (/s/) sound. Under normal circumstances, the duration of the voiceless sound should far exceed that of the voiced (the s/z ratio should be large), however when glottic insufficiency is current, the period tends to turn out to be approximately the same (the s/z ratio tends to decrease). Fundamentally, diagnostic testing in addition to the historical past and bodily examination is intended to uncover occult causes of vocal fold paralysis. In cases temporally associated to a surgery which places the vocal folds in danger, no additional workup is required. This includes the mediastinum and the pulmonary apex, even when the paralysis is rightsided; it must be recalled that the best recurrent laryngeal nerve loops beneath the subclavian artery. Although some authors have instructed that routine radiography may be adequate to picture the chest, Glazer and colleagues have instructed a sobering price of false negatives. Rehabilitation without arytenoid repositioning surgery would likely be suboptimal. In turn, outcome expectations are influenced by the obvious cause of the paralysis and the time that has elapsed since onset. A recent survey has advised that otorhinolaryngologists continue to get hold of serologies in most sufferers with vocal fold paralysis. The potential of morbidity associated to dysphagia is a key element in figuring out the need for remedy. It can present unambiguous evidence of denervation and reinnervation, but its utility in patients with vocal fold paralysis has been hotly debated. Patients with hemilaryngeal paralysis, especially of quick length, could simply be noticed. As with many interventions for this situation, the natural tendency of glottic insufficiency to improve over time makes it difficult to evaluate efficacy. Nevertheless, a skilled voice therapist might supply sufferers reassurance and perception into their situation and will help forestall or reverse harmful compensatory behaviors. The presence of severe dysphagia, historical past of aspiration pneumonia or noticed aspiration throughout scientific analysis (either radiologic or endoscopic) successfully trumps other elements and demands intervention. Patients may go for temporary aid of their signs, even when eventual recovery is anticipated. This is accomplished by injection of an absorbable bulking substance into the paralyzed vocal fold to improve the glottic insufficiency. Such substances embrace numerous collagen and hyaluronic acid preparations, micronized human dermis, autologous fats and carboxymethylcellulose-glycerine gel. Injection augmentation could also be performed by way of direct laryngoscopy within the working room or perorally or transcutaneously underneath topical anesthesia or superior laryngeal nerve block within the workplace, supplied the patient is cooperative and committed.
References
- Everingham L. The Parastomal hernia dilemma. World Council of Enterostomal Therapists J 1998;18:32-34.
- Lee WR, Marcus RB Jr, Sombeck MD, et al. Radiotherapy alone for carcinoma of the vagina: the importance of overall treatment time. Int J Radiat Oncol Biol Phys 1994;29(5):983-988.
- Campbell SG, Marrie TJ, Anstey R, et al: The contribution of blood cultures to the clinical management of adult patients admitted to the hospital with community-acquired pneumonia: a prospective observational study. Chest 123:1142-1150, 2003.
- Guglin M, Cutro R, Mishkin JD. Trastuzumab-induced cardiomyopathy. J Card Fail 2008;14:437-444.
- Adrie C, Adib-Conquy M, Laurent I, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a 'sepsis-like' syndrome. Circulation. 2002;106(5): 562-568.