

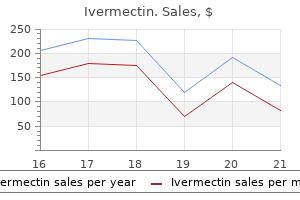
Ivermectin
Claire Bouvattier, MD
- MCU, Paris Descartes University
- PH,
- Cochin-Saint Vincent de Paul, Paris, France
Ivermectin dosages: 12 mg, 6 mg, 3 mg
Ivermectin packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Purchase ivermectin 3mg
Over time best antibiotic for uti yahoo answers ivermectin 3mg cheap, this induces adaptive mobile responses that are finally answerable for relieving despair virus living or not purchase 3mg ivermectin with mastercard. Symptoms embrace agitation antibiotic resistance not finishing prescription buy ivermectin 3mg fast delivery, confusion, hallucinations, hyperreflexia, tremor, and fever. Factors to assess embody have an effect on, thought content, interest in the surroundings, appetite, sleep patterns, and appearance. Reducing the Risk of Suicide Depression carries a threat of suicide, which may improve during the initial section of antidepressant therapy or when antidepressant dosage is modified. Preadministration Assessment Therapeutic Goal Alleviation of Symptoms of Major Depression. Arrange for the patient or care- giver to meet with the prescriber at least weekly in the course of the first 4 weeks of remedy, then biweekly for the next four weeks, then once 1 month later, and periodically thereafter. To forestall patients from accumulating a doubtlessly deadly provide of medication, be certain that every dose is swallowed and not "cheeked. Promoting Adherence make expectations extra sensible, which ought to assist promote adherence. Inform the patient that antidepressant effects normally develop slowly, over 1 to 3 weeks. Warn patients not to discontinue therapy once mood has improved, since doing so might result in relapse. Educate sufferers concerning the importance of taking their medication as prescribed, even though they may be symptom free and subsequently really feel "cured. Emotional support and psychotherapy can complement and reinforce responses to antidepressants. Evaluating Therapeutic Effects Assess patients for improvement in signs, particularly depressed temper and loss of curiosity or pleasure in usual actions. Symptoms of this probably fatal syndrome include agitation, confusion, disorientation, anxiety, hallucinations, poor focus, incoordination, myoclonus, hyperreflexia, extreme sweating, tremor, and fever. Inform sufferers about potential sexual dysfunction (anorgasmia, impotence, decreased libido), and encourage them to report issues. Managepatients to the sequelae of bruxism (headache, jaw ache, and dental problems, similar to cracked fillings). Minimizing Adverse Interactions tamines, glucocorticoids) or withdrawal of fluoxetine. Inform sufferers in regards to the danger of rash and instruct them to notify the prescriber if one develops. The danger of bleeding with warfarin is compounded by a pharmacokinetic interplay with fluoxetine, which can displace warfarin from binding websites on plasma proteins, causing ranges of free warfarin to rise. Preadministration Assessment Therapeutic Goal Alleviation of symptoms of main melancholy. Doxepin is contraindicated for sufferers with glaucoma or an inclination to urinary retention. If hypomania develops, the patient must be evaluated to decide if elation is drug induced or signifies bipolar disorder. Warn sufferers against utilizing alcohol and all anticholinergic medication (eg, scopolamine, antihistamines, phenothiazines). Once an efficient dosage has been established, the entire every day dose can usually be taken at bedtime. If blood pressure is low or pulse fee is high, withhold medicine and inform the prescriber. Inform patients about potential anticholinergic effects (dry mouth, blurred imaginative and prescient, photophobia, urinary hesitancy, constipation, tachycardia), and advise them to notify the prescriber if these are troublesome. Inform patients about symptoms of hypotension (dizziness, lightheadedness), and advise them to sit or lie down if these happen. Inform patients that hypotension could be minimized by moving slowly when assuming an erect posture. Preadministration Assessment Therapeutic Goal Alleviation of symptoms of major depression, particularly atypical despair. Advise patients to keep away from hazardous activities (eg, driving, working harmful machinery) if sedation is significant. Warn patients to not discontinue therapy as quickly as temper has improved, since doing so might end in relapse. Instruct sufferers to apply the Emsam patch to intact, dry pores and skin of the higher torso, upper thigh, or outer floor of the higher arm once each 24 hours. Inform sufferers about signs of hypertensive crisis- extreme headache, tachycardia, hypertension, nausea, vomiting, confusion, and profuse sweating-and instruct them to search instant medical consideration if these develop. Take these measurements whereas the affected person is lying down and once more after the affected person has been sitting or standing for 1 to 2 minutes. Application-site rash is common with transdermal selegiline, and can be managed with a topical glucocorticoid. Inform patients about indicators of hypotension (dizziness, lightheadedness), and advise them to sit or lie down if these happen. Manic individuals show overactivity at work and at play and have a lowered need for sleep. Extreme self-confidence, grandiose ideas, and delusions of self-importance are common. Manic people typically bask in high-risk actions (eg, questionable business offers, reckless driving, playing, sexual indiscretions), giving no forethought to the consequences. In extreme instances, signs could resemble these of paranoid schizophrenia (hallucinations, delusions, weird behavior). Associated symptoms embody disruption of sleeping and consuming patterns; problem concentrating; feelings of guilt, worthlessness, and helplessness; and thoughts of demise and suicide. In a real mixed episode, patients experience signs of mania and depression concurrently. Patients may be agitated and irritable (as in mania), but may also really feel worthless and depressed. The combination of high vitality and depression places them at important threat of suicide. The mainstays of remedy are lithium and divalproex sodium (valproate), medicine that may stabilize temper. Many patients additionally obtain an antipsychotic agent, and a few could require an antidepressant. Typically, patients expertise alternating episodes during which temper is abnormally elevated or abnormally depressed-separated by durations during which temper is comparatively normal. Symptoms usually begin in adolescence or early adulthood, but can happen before adolescence or as late because the fifth decade of life. In the absence of therapy, episodes of mania or depression usually persist for a quantity of months. Contrary to well-liked perception, not all sufferers alternate repeatedly between mania and depression.
Russian Penicillin (Propolis). Ivermectin.
- Dosing considerations for Propolis.
- Improving healing and reducing pain and inflammation after mouth surgery.
- What is Propolis?
- Are there safety concerns?
- How does Propolis work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96404
Cheap ivermectin 3mg mastercard
Given out as one of the two branches of the principle nerve simply above the inguinal ligament antibiotic resistance lab report quality 3 mg ivermectin, it passes deep to the inguinal ligament and enters the femoral sheath lateral to the femoral artery treatment for recurrent uti by e.coli best 3 mg ivermectin. It then pierces the anterior layer of the femoral sheath and fascia lata to attain the cutaneous plane antibiotics for uti and exercise discount ivermectin 3mg otc. The lateral cutaneous nerve of the thigh is seen close to the lateral angle of the femoral triangle. The anterior a half of this sleeve (forming the anterior wall) is contributed to by the transversalis fascia and the posterior part (forming the posterior wall) by the iliacus fascia. A little amount of extraperitoneal connective tissue also merges with these fasciae. This is the world of connection between the abdominal cavity and the femoral canal. The ring is bounded anteriorly by the inguinal ligament, medially by the crescentic edge of the lacunar ligament, posteriorly by the pectineus muscle and its fascia and laterally by the femoral vein. Its medial portion lies behind the saphenous opening and the lateral portion behind the fascia lata. The superior or proximal finish of the sheath is wider and open to the abdominal cavity. The inferior or distal end is narrower and merges with the perivascular connective tissue about 3 to four cm distal to the inguinal ligament. The lateral most compartment accommodates the femoral artery and the middle compartment accommodates the femoral vein. The medial most compartment, also the smallest, is recognized as the femoral canal It is occupied by a few lymphatic vessels and a lymph node (the lymph node of Cloquet or lacunar lymph node). Close to the anterior and anterolateral boundaries of the ring are the spermatic cord (or the round ligament) and the inferior epigastric vessels respectively. The ring is closed in life by a plate of extraperitoneal connective tissue; this plate known as the femoral septum. The apex of the triangle lies roughly 4 inches inferior to the inguinal ligament. The dominant structure throughout the body of the femoral triangle is the femoral artery. The artery runs along an internervous boundary-the boundary line that separates the territories of two motor nerves. The muscular tissues of the medial a part of the triangle are provided by the obturator nerve and those of the lateral half by the femoral nerve. The profunda femoris artery arises from the femoral artery normally 2 to 5 cm under the inguinal ligament. The femoral vein is posterior to the femoral artery on the degree of the apex of the triangle. Tough areolar tissue surrounds all the four vessels and all keep them united to each other the nice saphenous vein is the final tributary to be part of the femoral vein. The femoral nerve enters the thigh lateral to the artery but outdoors the fascia iliaca. The relationship of the femoral vessels and the nerve to the hip joint are necessary. The femoral sheath permits the femoral vessels to glide smoothly deep to the inguinal ligament throughout actions of the hip joint. The constructions which are in entrance of the hip joint are likely to bowstring throughout flexion; this is prevented by the inguinal ligament which retains the structures in position. Retroinguinal space: As the inguinal ligament bridges the gap between the pubic tubercle and the ante ior superior iliac backbone, a passageway between the stomach cavity and the thigh is created. This area is split into two compartments by a fascial partition known as the iliopectineal arch. The iliopectineal arch is a thickening of the medial portion of the iliacus fascia and runs from the deep aspect of inguinal ligament to the iliopubic eminence the compartment lateral to the iliopectineal arch is muscular; the iliopsoas muscle and the femoral nerve pass through this compartment. The compartment medial is vascular; the femoral vessels pass by way of it enclosed in the femoral sheath. If current, the muscle lies inside the abdomen however is intently related w th the psoas main. The rectus femoris and the three vasti together type the quadriceps femoris; they act on the knee joint by way of a typical tendon and therefore are thought-about as one muscle. Adductor longus and pectineus, that are muscular tissues of the medial compartment are sometimes grouped within the anterior compartment because of their presence in the front of thigh. Tensor fasciae latae is classed as a gluteal muscle by the clinicians Clinical Correlation s fre fre fre Femoral hernia: the femoral canal is a weak space ensuing within the incidence of femoral hernia. Abdominal viscera (usually a coil of small intestine) can p otrude through the femoral ring into the femoral canal. As the intraabdominal stress increases because of some cause, more and more of the length of the gut descends into the femoral canal. A small femoral hernia seems as a rounded mass in the femoral triangle inferolateral to the pubic tubercle. When the hernia turns into larger in dimension, it en arges beyond the dimensions of the femoral canal and passes via the saphenous opening (a passage easily available at this level) to reach the subcutaneous tissue. If the hernia will increase still further in dimension, it extends towards the anterior superior iliac backbone. Strangulation of femoral herniae are also commoner than that of other hernia; the boundaries of the femoral ring are inflexible and the medial margin (concave margin of the lacunar ligament) is especially sharp. While repairing the femoral hernia or whereas releasing a strangulated hernia, it might be essential to widen the neck of the hernial sac. On the lateral side of the ring is the femoral artery; attempting to meddle in that course could cause intensive bleeding and therefore, ought to be avoided. The anterior and posterior aspects have firm buildings within the type of the inguinal ligament and the superior pubic ramus respectively. Widening is possible only by slicing by way of the sharp concave border of the lacunar ligament. Sometimes this department is replaced by a pubic branch of the interior epigastric artery (called the changed obturator artery) or supplemented by the identical (the pubic department of the interior epigastric is then called an adjunct obturator artery); even then, most frequently, these arteries are away from the lacunar ligament. Rarely, either the changed or the accent obturator artery passes over the concave border of the lacunar ligament (named the aberrant obturator artery in such a case). This artery might inadvertently be reduce throughout hernial restore and trigger in depth bleeding. When the thigh is fixed, bilateral contraction of iliopsoas causes flexion of hip. Iliopsoas is actively involved in climbing downstairs and in upkeep of regular posture. Additional Notes on Sartorius It is the longest muscle within the body, being in the shape of a slim strap. Sartus= patching or repair; sartor=tailor) is derived from its efficacy in causing flexion at hip and knee concurrently which are required for a tailor in professing the occupation. The muscular tissues of this compartment (anterior thigh muscles) act as extensors of the hip and flexors of the knee. However, the compartment is identified as the extensor compartment, taking the action on the hip into consideration.
Order 3 mg ivermectin with visa
These three elements meet at the acetabulum antibiotics made simple ivermectin 3 mg lowest price, which is a big deep cavity positioned on the lateral aspect of the bone antibiotics gain weight purchase 3 mg ivermectin. The acetabulum takes half in forming the hip joint along with the head of the femur antibiotic resistance future ivermectin 3mg online. The posterior part of the ilium bears a big rough articular space on its medial aspect for articulation with the sacrum. The two pubic bones meet in the center line, in entrance to form the pubic symphysis. This place, during research, can be simply obtained fre Orientation of the Hip Bone by putting the bone against a wall. In this position, the ischial spine is above the superior degree of the symphysis and the coccygeal tip is under it. However, in vivo, in the males, the anterior superior iliac spines fall short of the vertical by about half inch. The anterior end of the iliac crest projects forwards as the anterior superior iliac backbone. The posterior finish of the crest additionally forms a projection called the posterior superior iliac spine. The iliac crest may be subdivided into a ventral phase, consisting of the anterior two-thirds of the crest, and a dorsal section consisting of the posterior one-third. The outer lip is most prominent and is about 5 cm behind the anterior superior iliac backbone. Posterior border of ilium: the posterior border of the ilium extends from the posterior superior iliac spine to the back of the acetabulum. A few centimetres beneath the posterior superior iliac backbone the posterior border presents another prominence known as the posterior inferior iliac spine. The lower part of the posterior border curves all the means down to type the boundary of a deep notch known as the larger sciatic notch. This floor is marked by three ridges called the posterior, anterior and inferior gluteal traces. It extends from the iliac crest above, to the posterior inferior iliac spine beneath. Its anterior end meets the iliac crest in entrance of the tubercle; while its posterior end reaches the greater sciatic notch. Its anterior end lies simply above the anterior inferior iliac spine; and its posterior finish reaches the greater sciatic notch. It may be subdivided into three parts- (1) the upper half which is rough and which constitutes the iliac tuberosity; (2) the center part called the auricular floor (because of its resemblance to the shape of pinna), which articulates with the lateral facet of the sacrum; (3) the smooth pelvic part, which lies beneath and in front of the auricular surface and takes part in forming the wall of the lesser pelvis. A tough groove referred to as the preauricular sulcus is often found (especially in females) in this space. The decrease a half of the gluteal surface extends behind the acetabulum the place it becomes steady with the ischium. The upper lateral part offers attachment to semimembranous muscle and is separated by an indirect line from the higher medial half which provides attachment to the semitendinosus and biceps femoris. The decrease lateral part offers attachment to the hamstrings part of sf re e fre Femoral floor: the femoral surface of the ischium is directed downwards, forwards and laterally. This border is sharp in its higher half the place it separates the iliac fossa from the auricular surface. The lower medial half is roofed by fibrous tissue and normally has an overlying bursa as a outcome of the pressure produced on sitting. The medial border of the tuberosity supplies attachment to the sacrotuberous ligament and the lateral border to the quadratus femoris muscle. The sacrotuberous ligament continues as a sickleshaped process (the falciform process) along the medial margin of the ischial ramus. Above this, the dorsal floor becomes continuous with the gluteal floor of the ilium. The posterior border of the dorsal floor of the ischium varieties part of the lower margin of the greater sciatic notch Just below this notch, the border projects backwards and medially as the ischial backbone. Between the ischial backbone and the higher border of the ischial tuberosity is the shallow lesser sciatic notch. It passes upwards and forwards to join the inferior ramus of pubis; the inferior pubic ramus and the ischial ramus together type the conjoined ischiopubic ramus. The inferior border is also sharp and forms the upper margin of the obturator foramen. The floor between the obturator crest and the pecten pubis is the pectineal surface. A groove runs forwards and downwards across it and is known as the obturator groove. In the intact pelvis, the conjoined rami of the pubis and isch um of the 2 sides type the boundaries of the pubic arch which lies under the pubic symphysis. The inferior ramus of the pubis has an anterior (or outer) floor, and a posterior (or inner) floor. The margin of the acetabulum is poor within the anteroinferior part and the gap within the margin known as the acetabular notch. The articular space for the head of femur is formed like a horseshoe and is called the lunate surface this floor is widest superiorly. The upper a half of the acetabulum varieties a projection on the decrease finish of ilium for weight transmission to femur. It is sure superiorly by the superior ramus of the pubis; medially by the body of the pubis, inferiorly by its inferior ramus and by the ramus of the ischium; and laterally by the physique of the ischium. In the intact physique, the foramen is filled by a fibrous sheet called the obturator membrane. The two endpoints the place the free edge joins the bone often have the anterior and posterior obturator tubercles. The inner indirect muscle of the stomach arises from the intermediate space of the ventral phase of the iliac crest. Gluteus maximus arises from the gluteal surface of the ilium behind the posterior gluteal line. Gluteus medius arises from the gluteal surface of the ilium between the anterior and posterior gluteal lines. The tensor fasciae latae arises from the anterior a half of the outer lip of the iliac crest. The transversus abdominis arises from the anterior two-thirds of the inner lip of the ventral phase of the iliac crest. The quadratus lumborum arises from the posterior one-third of the inner lip of the ventral segment of the iliac crest. The gluteus maximus arises from the lateral floor of the dorsal segment of the iliac crest (and from the gluteal surface of the ilium behind the posterior gluteal line). The erector spinae arises from the medial floor of the dorsal segment of the iliac crest.

Buy cheap ivermectin 3 mg online
Fentanyl sublingual tablets [Abstral] are available in six strengths: a hundred infection kidney buy 3mg ivermectin visa, 200 ear infection 1 year old best ivermectin 3 mg, 300 virus nucleus ivermectin 3 mg without a prescription, four hundred, 600, and 800 mcg. Patients should place the pill on the ground of the mouth instantly underneath the tongue, and allow it to dissolve utterly. No greater than two doses ought to be used for any ache episode, and sufferers ought to wait no less than 2 hours before dosing once more. With every subsequent episode, the dose must be titrated until a secure and effective dose is identified. Fentanyl nasal spray [Lazanda], approved in 2011, is much like transmucosal fentanyl. The spray must not be used for acute ache, postoperative pain, headache, or athletic accidents. As with the transmucosal products, the dose of fentanyl in Lazanda can be deadly to nontolerant individuals, so the spray have to be saved in a secure, child-resistant location. Intranasal fentanyl is supplied in 5-mL bottles which have a metered-dose nasal spray pump. If needed, dosage may be titrated upward at subsequent pain episodes as follows: 200 mcg (100 mcg in every nostril), four hundred mcg (400 mcg in 1 nostril), after which 800 mcg (400 mcg in 2 nostrils). If more than 5 days elapse for the reason that final dose, the bottle must be discarded and replaced with a model new one. Fentanyl for transmucosal administration is on the market in five formulations: lozenges on a stick [Actiq], buccal film [Onsolis], buccal tablets [Fentora], sublingual spray [Subsys], and sublingual tablets [Abstral]. Transmucosal fentanyl must not be used for acute pain, postoperative pain, headache, or athletic accidents. Adverse results of transmucosal fentanyl are like those of different opioid preparations. The most typical are dizziness, anxiety, confusion, nausea, vomiting, constipation, dyspnea, weak spot, and headache. For instance, a 100-mcg buccal tablet produces about the same fentanyl blood degree as does a 200-mcg lozenge. To administer the unit, sufferers place it between the cheek and the lower gum and actively suck it. Analgesia begins in 10 to 15 minutes, peaks in 20 minutes, and persists 1 to 2 hours. If breakthrough pain persists, the patient can take another 200-mcg unit quarter-hour after finishing the primary one (ie, half-hour after starting the first). If the affected person needs more than 4 units/day, it may be time to give a better dose of his or her long-acting opioid. To promote secure and effective use of the Actiq system, the manufacturer provides an Actiq Welcome Kit as well as a Child Safety Kit with the preliminary drug supply. The package incorporates academic materials and secure storage containers for unused, partially used, and completely used units. Fentanyl buccal film [Onsolis] is made utilizing a drug-delivery technology often recognized as BioErodible MucoAdhesive. A single dose of the movie is about 1 cm sq. and really skinny, with a pink side (that delivers the fentanyl) and a white side (that signifies the strength). Patients ought to press the pink side against the inside of the cheek for five seconds, after which Alfentanil and Sufentanil Alfentanil [Alfenta] and sufentanil [Sufenta] are intravenous opioids related to fentanyl. Both drugs are used for induction of anesthesia, for upkeep of anesthesia (in combination with other agents), and as sole anesthetic agents. Sufentanil has an especially high milligram potency (about a thousand occasions that of morphine). Remifentanil Remifentanil [Ultiva] is an intravenous opioid with a fast onset and brief period. The transient period outcomes from speedy metabolism by plasma and tissue esterases, and not from hepatic metabolism or renal excretion. Remifentanil is approved for analgesia during surgery and in the course of the quick postoperative period. Effects start in minutes, and terminate 5 to 10 minutes after the infusion is stopped. Adverse results in the course of the infusion embody respiratory melancholy, hypotension, bradycardia, and muscle rigidity adequate to compromise breathing. Meperidine Meperidine [Demerol] shares the major pharmacologic properties of morphine. Meperidine was once considered a first-line drug for reduction of average to severe pain. First, the drug has a brief half-life, so dosing have to be repeated at quick intervals. The underlying mechanism seems to be extreme activation of serotonin receptors owing to meperidine-induced blockade of serotonin reuptake. Repeated dosing results in accumulation of normeperidine, a toxic metabolite that can trigger dysphoria, irritability, tremors, and seizures. There have been rising reviews of deaths and life-threatening unwanted effects (especially dysrhythmias and respiratory depression) among sufferers taking methadone to relieve ache. The presumed cause of toxicity is high drug ranges, owing largely to excessive dosage. In addition, the drug is out there in dispersible 40-mg tablets for detoxification and upkeep of opioid addicts. All oxymorphone tablets should be taken on an empty abdomen, as a end result of dosing with food can produce excessive peak ranges. Also, alcohol ought to be averted, since it may possibly increase blood levels of oral oxymorphone. Moderate to Strong Opioid Agonists the moderate to robust opioid agonists are just like morphine in most respects. Differences between the average to strong opioids and morphine are primarily quantitative: the moderate to strong opioids produce much less analgesia and respiratory depression than morphine and have a somewhat decrease potential for abuse. As with morphine, toxicity from the moderate to sturdy agonists may be reversed with naloxone. All three medication are robust opioid agonists with pharmacologic actions like those of morphine, and all three are indicated for average to severe ache. Adverse effects embrace respiratory despair, sedation, cough suppression, Codeine Codeine is indicated for aid of mild to moderate ache. As a end result, although taking codeine can produce significant pain aid, the degree of pain reduction that may be achieved safely is kind of low-much decrease than with morphine. When taken in its traditional analgesic dose (30 mg), codeine produces about as much pain relief as 325 mg of aspirin or 325 mg of acetaminophen. In the liver, about 10% of every dose of codeine undergoes conversion to morphine, the energetic type of codeine.
Generic ivermectin 3mg visa
The deeper layer passes deep to the tensor fasciae latae and blends with the lateral part of the capsule of the hip joint antibiotics for urinary tract infection in dogs generic ivermectin 3 mg online. The tensor fascia latae and the gluteus maximus muscular tissues contribute to a set of vertical fibres which descend between the two sets of round fibres and kind the bulk of the tract antibiotic linezolid discount ivermectin 3mg otc. The space of attachment of the iliotibial tract to the tibia types a distinguished triangular impression on the anterolateral aspect of the lateral tibial condyle bone antibiotics for sinus infection without penicillin 3mg ivermectin. An aponeurotic growth from the vastus lateralis merges with the iliotibial tract right here. The tract stands out as a outstanding ridge on the anterolateral facet of the knee when the leg is prolonged. Saphenous opening: An opening in a sheet or fascia is usually a deficit within the structure. The opening is formed not because a small portion of the fascia is missing but as a result of the 2 strata of the fascia have overlapped. It is to be imagined just like the gap created when the right and left flaps of the front of a coat are overlapped. This rim varieties the superior, lateral and inferior curves of the saphenous opening and is identified as the falciform margin. The superior and inferior curves are also called the superior and inferior cornua. The decrease rim of the deep stratum continues from the inferior cornu and extends superolaterally covering the pectineus, adductor longus and gracilis muscle tissue. The deep stratum gets connected to the pubic tubercle and the pecten pubis of the superior pubic ramus. The saphenous opening is under and lateral to the medial part of the inguinal ligament; the centre of the opening is about three cm inferior and lateral to the pubic tubercle. The opening is closed by the cribriform fascia which is half of the superficial fascia. The cribriform fascia is connected to the falciform margin on the lateral side; on the medial aspect it merges imperceptibly with the deep stratum. The nice saphenous vein pierces the cribriform fascia and passes through the saphenous opening to be a part of the femoral vein. A little beneath, the sleeve regains its cylindrical type the inferior ring of attachment is along the patella, the lateral femoral and tibial condyles, the capsule of the knee joint and the medial femoral and tibial condyles. The fascia lata along its inferior ring of attachment becomes steady with the deep fascia of the leg. Since the fascia lata is connected to the iliac crest and the sacrotuberous ligament, it covers the gluteal muscle tissue too. That a part of the deep fascia which is over the gluteal muscular tissues is sometimes called the gluteal fascia and the name fascia lata is normally restricted to the deep fascia of the thigh correct. When the fascia descends over the gluteus medius from the iliac crest, it splits into two as it reaches the higher border of gluteus maximus. One of the layers passes superficial to the muscle and the other deep to the muscle to reunite at its decrease border. The superficial stratum of the fascia lata is anterior to the femoral sheath and merges with the anterior layer of the sheath. The deep stratum is posterior to the femoral sheath however separated from it by free connective tissue. The boundaries of the triangle are as follows: the superior boundary or base is the inguinal ligament; the lateral boundary is the medial margin of sartorius; the medial boundary is the medial margin of adductor longus; the apex is the place the medial and the lateral borders meet. The floor of the triangle is fashioned (from lateral to medial side) by the iliacus, the psoas main, the pectineus and the adductor longus muscular tissues. The roof is formed by the fasciae over the region and the superficial buildings within them. These embrace the saphenous opening, the cribriform fascia, the terminal part of the saphenous vein and the superficial inguinal lymph nodes. Disposition of the various muscular tissues leads to the formation of a muscular triangle called the femoral triangle within the upper a part of anterior thigh. The compartment really encircles most of the shaft of the femur and consists of bulky muscular tissues. The medial compartment, in any other case referred to as the adductor compartment or the obturator compartment, lies behind the medial intermuscular septum and in entrance of the posterior intermuscular septum Though the 2 compartments are described individually, the muscular tissues of both the compartments are seen collectively on removal of deep fascia within the entrance of thigh. Running diagonally throughout the thigh from the lateral to the medial side is the skinny and lengthy muscle called the sartorius. Running downwards along the lateral margin of the higher a half of the thigh are the tensor fasciae latae and the iliotibial tract. Parts of a large muscle called the quadriceps femoris are seen between the sartorius and the tensor fasciae latae. That part of the quadriceps operating roughly vertically down the centre of the thigh is the rectus femoris. To the lateral aspect of the rectus femoris is the vastus lateralis; to the medial facet of the rectus femoris is the vastus medialis. Deep to rectus femoris, vastus medialis and vastus lateralis is the vastus intermedius the rectus and the three vasti collectively kind the quadriceps. The area medial to the sartorius and beneath the level of the psoas main is occupied by a number of muscle belonging to the medial compartment of the thigh. The anterior division gives off a muscular branch to the sartorius muscle, the medial and intermediate cutaneous nerves of the thigh. The posterior division gives off muscular branches to the rectus femoris, vastus lateralis, vastus intermedius and vastus medialis and a large sensory branch known as the saphenous nerve. These are the (a) superficial circumflex iliac artery, (b) superficial epigastric artery and (c) superficial exterior pudendal artery. A quick distance beneath the inguinal ligament, two different branches are given off: a. The higher finish of the femoral vein lies medial to the femoral artery However, at the apex of the femoral triangle, the vein lies posterior to the artery. Other tributaries of the femoral vein correspond to branches of the femoral artery. After a short course of just about an inch within the femoral triangle, the femoral nerve divides into anterior and fre fre the femoral artery which runs down the center of the triangle, from midbase to the apex and a few of its branches; the femoral vein which has a close however twisted relationship to the artery; the femoral nerve which is a short distance lateral to the artery and some of its branches; the deep inguinal lymph nodes; the profunda femoris and the circumflex vessels. The posterior abdominal wall has the iliacus and psoas major muscle tissue on its internal side. They are coated by a fascia referred to as the iliopsoas fascia (or merely, the iliac fascia) on their anterior elements. The iliopsoas passes behind the inguinal ligament into the thigh from the abdomen. On the anterior facet, the innermost muscle of the anterior belly wall is the transverses abdominis; this muscle is lined by the transversalis fascia. It is of course expected that on the decrease side of the trunk, the anterior and posterior partitions would come towards each other and join to shut off the body cavity. In such a case, the transversalis fascia from the anterior facet and the iliac fascia from the posterior aspect would also be a part of together and seal the cavity. The femoral sheath is a funnel-shaped fibroareolar construction that wraps around the femoral vessels within the upper a half of the thigh.
Cheap 3 mg ivermectin with mastercard
To cut back the chance of serious hematologic results 0x0000007b virus buy ivermectin 3mg cheap, (1) acquire complete blood counts at baseline and periodically thereafter antibiotics for acne safe 3 mg ivermectin sale, (2) avoid carbamazepine in patients with preexisting hematologic abnormalities infection hair follicle discount ivermectin 3mg fast delivery, and (3) inform patients about manifestations of hematologic abnormalities (fever, sore throat, pallor, weakness, an infection, easy bruising, petechiae), and instruct them to notify the prescriber if these happen. Phenytoin can decrease the consequences of these agents (as properly as other drugs) by inducing hepatic drug-metabolizing enzymes. Preadministration Assessment Therapeutic Goal Carbamazepine is used to treat partial seizures (simple and complex) and tonic-clonic seizures. Identifying High-Risk Patients Carbamazepine is contraindicated for sufferers with a history of bone marrow melancholy or antagonistic hematologic reactions to other medication. Administration Advise patients to administer carbamazepine with meals to decrease gastric upset. Use in being pregnant provided that the benefits of seizure suppression outweigh the risks to the fetus. Patients using these medication would require elevated dosages to preserve therapeutic responses. These medication can decrease responses to carbamazepine by inducing drugmetabolizing enzymes (beyond the degree of induction attributable to carbamazepine itself). Preadministration Assessment Therapeutic Goal Valproic acid is used to deal with all main seizure issues: tonic-clonic, absence, myoclonic, atonic, and partial (simple, advanced, and secondarily generalized). Administration Advise sufferers to take valproic acid with meals, and instruct them to ingest tablets and capsules intact, without crushing or chewing. Levels of phenobarbital and phenytoin must be monitored and their dosages adjusted accordingly. Nursing implications that apply to the barbiturates as a bunch are summarized in Chapter 34. Preadministration Assessment Therapeutic Goal Oral phenobarbital is used for partial seizures (simple and complex) and tonic-clonic seizures. Identifying High-Risk Patients Phenobarbital is contraindicated for sufferers with a history of acute intermittent porphyria. Ongoing Evaluation and Interventions Minimizing Adverse Effects Neuropsychologic Effects. Inform dad and mom that kids could become irritable and hyperactive, and instruct them to notify the prescriber if these behaviors happen. Inform patients about signs of pancreatitis If pancreatitis is recognized, valproic acid ought to be withdrawn. Valproic acid may trigger neural tube defects and other congenital malformations, especially when taken in the course of the first trimester. Advise (abdominal ache, nausea, vomiting, anorexia) and instruct them to get an instantaneous evaluation if these develop. These may be decreased by using an enteric-coated formulation (see Table 24�4) and by taking valproic acid with meals. If signs develop (vomiting, lethargy, altered stage of consciousness and/or cognitive function), blood ammonia ought to be measured. If the extent is extreme, both valproic acid or topiramate must be withdrawn. Effects on oral contraceptives and warfarin are a specific concern; their dosages should be elevated. Minimizing Adverse Interactions enzymes, and can thereby lower responses to different medicine. Tizanidine promotes inhibition by appearing as an agonist at presynaptic alpha2 receptors. Spasm may end up from quite so much of causes, including epilepsy, hypocalcemia, acute and persistent ache syndromes, and trauma (localized muscle injury). Physical measures include immobilization of the affected muscle, software of cold compresses, whirlpool baths, and bodily therapy. For drug therapy, two teams of medicines are used: (1) analgesic antiinflammatory brokers (eg, aspirin), and (2) centrally acting muscle relaxants. Therapeutic Use the centrally appearing muscle relaxants are used to relieve localized spasm resulting from muscle damage. These agents can lower native ache and tenderness and can improve range of motion. Benefits of remedy equal those of aspirin and the opposite analgesic antiinflammatory medicine. Liver operate should be assessed before starting treatment and periodically thereafter. Chronic, high-dose remedy could cause bodily dependence, manifesting as a probably lifethreatening abstinence syndrome if these medication are abruptly withdrawn. Cyclobenzaprine and orphenadrine have significant anticholinergic (atropine-like) properties, and therefore may cause dry mouth, blurred imaginative and prescient, photophobia, urinary retention, and constipation. Methocarbamol could flip urine brown, black, or dark green; sufferers ought to be forewarned of this harmless impact. Tizanidine could cause dry mouth, hypotension, hallucinations, and psychotic symptoms. Carisoprodol may be Mechanism of Action For most centrally performing muscle relaxants, the mechanism of spasm reduction is unclear. At the dosage required to have adequate impact, sedation creates an increased fall danger. In addition, older adults are more delicate to benzodiazepines than youthful patients. These drugs could cause sedation and cognitive impairment, thus creating a fall risk. Longacting benzodiazepines such as diazepam are particularly troublesome as a outcome of older-adult patients tend to have a slower metabolism. Baclofen Mechanism of Action Baclofen [Lioresal, Gablofen] acts throughout the spinal twine to suppress hyperactive reflexes concerned in regulation of muscle motion. Therapeutic Use Baclofen can reduce spasticity related to multiple sclerosis, spinal twine injury, and cerebral palsy-but not with stroke. The drug decreases flexor and extensor spasms and suppresses resistance to passive motion. These actions scale back the discomfort of spasticity and permit elevated efficiency. These responses are most intense in the course of the early phase of remedy and diminish with continued drug use. Abrupt withdrawal of oral baclofen can cause visual hallucinations, paranoid ideation, and seizures. Potential reactions embrace excessive fever, altered mental standing, exaggerated rebound spasticity, and muscle rigidity that, in rare cases, has advanced to rhabdomyolysis (muscle breakdown), multiple organ system failure, and dying. To keep away from these severe penalties, the infusion system have to be programmed correctly and carefully monitored. Dosage and Administration All centrally appearing skeletal muscle relaxants may be administered orally (Table 25�1). These problems are characterised by heightened muscle tone, spasm, and loss of dexterity. Two of these-baclofen and diazepam-act Preparations, Dosage, and Administration Oral.
Syndromes
- Abdominal pain, changes in bowel movements, or weight loss
- Wheezing
- Angioplasty and stent placement
- Certain cancers
- Electrode patches are placed on the front and back of the chest and connected to the defibrillator.
- Do you have pain?
- Amputations
- Chest x-ray
- Normal eye pressure
- Almost all multivitamins. Vitamin B12 is better absorbed by the body when it is taken along with other B vitamins, such as niacin, riboflavin, vitamin B6, and magnesium.
Buy discount ivermectin 3mg on line
Identifying High-Risk Patients Use all dopamine agonists with caution in older-adult sufferers and in those with psychiatric problems antibiotics for steroid acne buy 3 mg ivermectin visa. Use pramipexole and ropinirole with warning in patients prone to antibiotics for sinus infection and breastfeeding safe 3mg ivermectin compulsive habits antibiotics kill candida buy ivermectin 3mg otc. Inform sufferers that nausea and vomiting could be reduced by taking oral dopamine agonists with meals. Instruct patients to notify the prescriber if nausea and vomiting persist or turn out to be severe. Instruct sufferers taking apomorphine to pretreat with trimethobenzamide [Tigan], an antiemetic. Inform patients about symptoms of orthostatic hypotension (dizziness, lightheadedness on standing) and advise them to sit or lie down if these happen. Inform sufferers about possible motion disorders (tremor, dystonic movements, twitching) and instruct them to notify the prescriber if these develop. Forewarn sufferers that dopamine agonists may cause hallucinations, especially in older adults, and instruct them to notify the prescriber if these develop. Warn sufferers that pramipexole, ropinirole, rotigotin, and apomorphine could cause sleep assaults. Instruct patients that, if a sleep assault occurs, they should inform the prescriber and avoid probably hazardous activities (eg, driving). Inform patients of child-bearing age that ropinirole may hurt the growing fetus, and advise them to use efficient birth control. If pregnancy occurs and will pramipexole, Inform sufferers that oral dopamine agonists could additionally be taken with food to scale back nausea and vomiting. To minimize opposed results, dosage must be low initially and then progressively increased. Pramipexole and ropinirole might induce compulsive, self-rewarding behaviors, including compulsive gambling, eating, buying, and hypersexuality. Risk factors include relative youth, a household or private historical past of alcohol abuse, and a novelty-seeking persona. Before prescribing these medication, clinicians ought to display screen patient for compulsive behaviors. First, acetylcholine is a crucial transmitter in the hippocampus and cerebral cortex, areas the place neuronal degeneration occurs. Second, acetylcholine is critical to forming memories, and its decline has been linked to reminiscence loss. It is the sixth main cause of demise, with an annual cost of about $203 billion. Major pathologic findings are cerebral atrophy, degeneration of cholinergic neurons, and the presence of neuritic plaques and neurofibrillary tangles-all of which begin to develop years before clinical symptoms appear. These spherical our bodies are composed of a central core of beta-amyloid (a protein fragment) surrounded by neuron remnants. The underlying trigger is manufacturing of an abnormal type of tau, a protein that, in healthy neurons, forms cross-bridges between microtubules, and thereby keeps their configuration stable. The cerebral cortex is central to speech, notion, reasoning, and different larger features. These include complete loss of speech, loss of bladder and bowel management, and complete lack of ability for self-care. Between 70% and 90% finally develop conduct problems (wandering, pacing, agitation, screaming). All sense of identity is misplaced and the individual is totally dependent on others for survival. Other attainable threat factors include head harm, low educational level, manufacturing of apoE4, high ranges of homocysteine, low ranges of folic acid, estrogen/progestin therapy, sedentary life-style, and nicotine in cigarette smoke. Symptoms usually start after age 65 years, however might appear in folks as younger as 40 years. At best, medicine currently in use could gradual lack of reminiscence and cognition, and extend independent operate. Three of the drugs-donepezil, galantamine, and rivastigmine- are cholinesterase inhibitors. As one expert put it, advantages of those drugs are equivalent to dropping half a pound after taking a weight reduction drug for six months: the loss could additionally be statistically important, nevertheless it has little scientific significance. No single drug is more practical than the others, so selection must be based on tolerability, ease of use, and price. Properties of the cholinesterase inhibitors and memantine are shown in Table 22�2. Reduce dosage in sufferers with moderate hepatic or renal impairment, and discontinue in sufferers with extreme hepatic or renal impairment. Reduce dosage in patients with average renal impairment and discontinue in patients with severe renal impairment. Cholinesterase Inhibitors the cholinesterase inhibitors were the primary medication approved by the U. In scientific trials, these drugs produced modest enhancements in cognition, behavior, and performance, and barely delayed disease development. All cholinesterase inhibitors are permitted for sufferers with mild to moderate signs, and one agent-donepezil-is also approved for these with extreme symptoms. Among those that do benefit, improvements are seen in quality of life and cognitive functions (eg, reminiscence, thought, reasoning). Nonetheless, although improvements are neither universal, dramatic, nor lengthy lasting, and though unwanted effects are frequent, the benefits may still be definitely value the risks for some patients. Elevation of acetylcholine at synapses in the lungs can cause bronchoconstriction. Increased activation of cholinergic receptors within the heart can cause symptomatic bradycardia, leading to fainting, falls, fall-related fractures, and pacemaker placement. If a patient is experiencing bradycardia, fainting, or falls, drug withdrawal may be indicated, especially if cognitive advantages are lacking. Drugs that block cholinergic receptors (eg, first-generation antihistamines, tricyclic antidepressants, conventional antipsychotics) can scale back therapeutic results, and should be prevented. Dosage ought to be carefully titrated, and therapy ought to proceed as long as clinically indicated. The highest doses produce the best benefits-but additionally the most intense unwanted aspect effects. Accordingly, dosage must be low initially after which progressively increased to the best tolerable quantity. Treatment can continue indefinitely, or till unwanted facet effects become insupportable or benefits are lost. Accordingly, choice among them relies on unwanted side effects, ease of dosing, and cost. Donepezil is nicely absorbed following oral administration and undergoes metabolism by hepatic cytochrome P450 enzymes. With all formulations, dosage must be adjusted in patients with hepatic or renal impairment as follows: For those with moderate hepatic or renal impairment, the maximum dosage is sixteen mg/ day; for these with extreme hepatic or renal impairment, galantamine ought to be avoided.
Cheap ivermectin 3mg free shipping
Some frequent mnemonics may help you to identify these doubtlessly dangerous circumstances antibiotic lawsuit discount 3 mg ivermectin with visa. Intravenous atropine can alleviate the muscarinic effects of cholinesterase inhibition antibiotics and birth control buy discount ivermectin 3mg line. Edrophonium and Pyridostigmine Edrophonium [Enlon] and pyridostigmine [Mestinon] have pharmacologic results very like these of neostigmine infection red line buy ivermectin 3 mg lowest price. One of those drugs-edrophonium- is noteworthy for its very transient duration of action. Although these medication can be cut up from cholinesterase, the splitting reaction takes place extraordinarily slowly. Hence, beneath normal conditions, their binding to cholinesterase can be considered irreversible. Because binding is irreversible, results persist till new molecules of cholinesterase may be synthesized. Although we usually consider the bond between irreversible inhibitors and cholinesterase permanent, this bond can, actually, be broken. To break the bond and reverse the inhibition of cholinesterase, we should administer pralidoxime, a cholinesterase reactivator. Pharmacologic Effects the irreversible cholinesterase inhibitors produce essentially the identical spectrum of results as the reversible inhibitors. The principal distinction is that responses to irreversible inhibitors final a long time, whereas responses to reversible inhibitors are transient. Therapeutic Uses the irreversible cholinesterase inhibitors have just one indication: treatment of glaucoma. The limited indications for irreversible cholinesterase inhibitors should be no surprise given their potential for harm. Because of this phosphorus atom, the irreversible inhibitors are often identified as organophosphate cholinesterase inhibitors. Easy absorption, coupled with high toxicity, is what makes these drugs good insecticides-and provides them potential as agents of chemical warfare. Agricultural employees have been poisoned by accidental ingestion of organophosphate pesticides and by absorption of those lipidsoluble compounds by way of the skin. In addition, because organophosphate pesticides are readily available to the basic public, poisoning could occur by chance or from tried homicide or suicide. Exposure may also occur if these medicine had been used as instruments of warfare or terrorism (see Chapter 110). Toxic doses of irreversible cholinesterase inhibitors produce cholinergic disaster, a situation characterised by extreme muscarinic stimulation and depolarizing neuromuscular blockade. Because of this atom, these medication are generally recognized as organophosphate cholinesterase inhibitors. With the exception of echothiophate, all of these medicine are extremely lipid soluble, and therefore transfer throughout the physique with ease. In poisoning by irreversible inhibitors, benefits derive from inflicting the inhibitor to dissociate from the energetic center of cholinesterase. Pralidoxime is way much less efficient at reversing cholinesterase inhibition at muscarinic and ganglionic websites. To be effective, pralidoxime have to be administered soon after organophosphate poisoning has occurred. In this process, the bond between the organophosphate inhibitor and cholinesterase increases in energy. Once getting older has occurred, pralidoxime is unable to trigger the inhibitor to dissociate from the enzyme. Intravenous doses should be infused slowly (over 20 to 30 minutes) to keep away from hypertension. Dosing intervals are individualized in accordance with severity and persistence of symptoms. Pralidoxime is out there alone beneath the trade name Protopam, and together with atropine beneath the trade names DuoDote and Atnaa. Rather, they solely produce symptomatic reduction, so sufferers normally want therapy lifelong. Accordingly, you want to assess the power to swallow earlier than giving oral medicines. If the patient is unable to swallow the water, parenteral medication must be substituted for oral medication. Dosage determination is achieved by administering a small initial dose adopted by additional small doses until an optimal level of muscle operate has been achieved. Important signs of enchancment include elevated ease of swallowing and increased capability to elevate the eyelids. You can help establish a correct dosage by preserving data of (1) times of drug administration, (2) times at which fatigue happens, (3) the state of muscle strength earlier than and after drug administration, and (4) signs of excessive muscarinic stimulation. To preserve optimal responses, sufferers must sometimes modify dosage themselves. To do this, they must be taught to acknowledge indicators of undermedication (ptosis, problem in swallowing) and signs of overmedication (excessive salivation and other muscarinic responses). For instance, they may find it essential to take supplementary medication 30 to 60 minutes before actions similar to eating or shopping. Usual grownup dosages for the brokers used to treat myasthenia gravis are � Neostigmine-15 to 375 mg/day in divided doses � Pyridostigmine-60 to 1500 mg/day in divided doses Myasthenic Crisis. Left untreated, myasthenic disaster can end result in death from paralysis of the muscle tissue of respiration. As famous beforehand, overdose with a cholinesterase inhibitor can produce cholinergic disaster. Like myasthenic disaster, cholinergic disaster is characterised by excessive muscle weak point or frank paralysis. In addition, cholinergic disaster is accompanied by signs of excessive muscarinic stimulation. The offending cholinesterase inhibitor should be withheld till muscle energy has returned. Common symptoms embody ptosis (drooping eyelids), issue swallowing, and weak spot of skeletal muscles. Reversible cholinesterase inhibitors (eg, neostigmine) are the mainstay of remedy. By stopping acetylcholine inactivation, anticholinesterase agents can intensify the effects of acetylcholine released from motor Distinguishing Myasthenic Crisis from Cholinergic Crisis. A historical past of medication use or signs of excessive muscarinic stimulation are normally adequate to permit a differential prognosis.
Order ivermectin 3mg
As a result of transmitter-receptor binding treatment for dogs eating cane toads discount ivermectin 3mg without a prescription, a series of occasions is initiated within the postsynaptic cell infection control policy purchase 3mg ivermectin, leading to antibiotic yeast cheap ivermectin 3mg with amex a change in its conduct. The precise nature of the change depends on the identification of the neurotransmitter and the kind of cell involved. If the postsynaptic cell is one other neuron, it could enhance or lower its firing rate; if the cell is a part of a muscle, it may contract or loosen up; and if the cell is glandular, it may increase or decrease secretion. Neuropharmacology can be outlined as the examine of drugs that alter processes managed by the nervous system. Neuropharmacologic medication produce results equal to these produced by excitation or suppression of neuronal exercise. The neuropharmacologic medicine constitute a big and essential family of therapeutic agents. These drugs are used to treat situations ranging from melancholy to epilepsy to hypertension to asthma. The clinical significance of these agents is mirrored in the fact that over 25% of this text is dedicated to them. The answer lies in a concept discussed in Chapter 5: Most therapeutic brokers act by serving to the physique assist itself. That is, most drugs produce their therapeutic results by coaxing the body to perform normal processes in a trend that advantages the patient. Since the nervous system participates in the regulation of practically all bodily processes, practically all bodily processes could be influenced by medication that alter neuronal regulation. Given the broad spectrum of processes that neuropharmacologic medication can alter, and given the potential advantages to be gained by manipulating those processes, it must be no surprise that neuropharmacologic medication have widespread scientific functions. Because drugs that alter synaptic transmission can produce effects which are rather more selective than these produced by medicine that alter axonal conduction. Recall that the method of conducting an impulse along an axon is basically the same in all neurons. As a consequence, a drug that alters axonal conduction will affect conduction in all nerves to which it has access. Because these agents produce nonselective inhibition of axonal conduction, they suppress transmission in any nerve they attain. Hence, though native anesthetics are certainly useful, their indications are restricted. Synaptic Transmission In distinction to medicine that alter axonal conduction, medication that alter synaptic transmission can produce results that are highly selective. In addition, for many transmitters, the body employs more than one type of receptor. Hence, through the use of a drug that selectively influences a selected kind of neurotransmitter or receptor, we are ready to alter one neuronally regulated course of while leaving most others unchanged. Because of their relative selectivity, medicine that alter synaptic transmission have many makes use of. Receptors the flexibility of a neuron to affect the conduct of another cell depends, ultimately, upon the power of that neuron to alter receptor exercise on the target cell. As mentioned, neurons alter receptor activity by releasing transmitter molecules, which diffuse throughout the synaptic gap and bind to receptors on the postsynaptic cell. If the goal cell lacked receptors for the transmitter that a neuron launched, that neuron can be unable to affect the goal cell. The effects of neuropharmacologic drugs, like these of neurons, depend on altering receptor activity. This commonsense concept is central to understanding the actions of neuropharmacologic drugs. Step 3, Release of transmitter: In response to an action potential, vesicles fuse with the terminal membrane and discharge their contents into the synaptic gap. Step four, Action at receptor: Transmitter binds (reversibly) to its receptor on the postsynaptic cell, causing a response in that cell. Step 5, Termination of transmission: Transmitter dissociates from its receptor and is then removed from the synaptic gap by (a) reuptake into the nerve terminal, (b) enzymatic degradation, or (c) diffusion away from the hole. For synaptic transmission to happen, molecules of transmitter must be current in the nerve terminal. In the determine, the letters Q, R, and S symbolize the precursor molecules from which the transmitter (T) is made. Transmitter storage takes place within vesicles-tiny packets present in the axon terminal. Release of transmitter is triggered by the arrival of an action potential at the axon terminal. The motion potential initiates a process in which vesicles bear fusion with the terminal membrane, inflicting launch of their contents into the synaptic hole. Each action potential causes only a small fraction of all vesicles present in the axon terminal to discharge their contents. Following release, transmitter molecules diffuse across the synaptic gap and then undergo reversible binding to receptors on the postsynaptic cell. This binding initiates a cascade of occasions that result in altered habits of the postsynaptic cell. Transmission is terminated by dissociation of transmitter from its receptors, followed by removal of free transmitter from the synaptic gap. Transmitter could be removed from the synaptic gap by three processes: (1) reuptake, (2) enzymatic degradation, and (3) diffusion. Following reuptake, molecules of transmitter may be degraded, or they may be packaged in vesicles for reuse. In synapses the place transmitter is cleared by enzymatic degradation (Step 5b), the synapse accommodates massive quantities of transmitter-inactivating enzymes. Although simple diffusion away from the synaptic gap (Step 5c) is a potential technique of terminating transmitter motion, this process could be very slow and generally of little significance. Termination of transmission Drug Action Increased synthesis of T Decreased synthesis of T Synthesis of "super" T Reduced storage of T Promotion of T release Inhibition of T release Direct receptor activation Enhanced response to T Blockade of T binding Blockade of T reuptake Inhibition of T breakdown Impact on Receptor Activation* Increase Decrease Increase Decrease Increase Decrease Increase Increase Decrease Increase Increase Effects of Drugs on the Steps of Synaptic Transmission As emphatically famous, all neuropharmacologic agents (except native anesthetics) produce their results by immediately or not directly altering receptor activity. We also noted that the way by which medication alter receptor activity is by interfering with synaptic transmission. Because synaptic transmission has a quantity of steps, the method presents numerous potential targets for medicine. In this section, we study the particular methods during which medicine can alter the steps of synaptic transmission. Before discussing specific mechanisms by which medicine can alter receptor activity, we have to understand what medicine are able to doing to receptors in general terms. From the broadest perspective, when a drug influences receptor function, that drug can do just considered one of two things: it can improve receptor activation, or it can cut back receptor activation. For our purposes, we can outline activation as an impact on receptor function equal to that produced by the natural neurotransmitter at a particular synapse. Hence, a drug whose results mimic the results of a natural transmitter would be said to enhance receptor activation. Conversely, a drug whose effects were equal to lowering the quantity of natural transmitter obtainable for receptor binding can be stated to lower receptor activation. For instance, a drug that mimics acetylcholine at receptors on the center will trigger the center to beat more slowly.
Discount 3 mg ivermectin free shipping
Preferred medication for prophylaxis embrace propranolol divalproex virus nyc generic ivermectin 3mg without a prescription, and amitriptyline virus 63 trusted 3 mg ivermectin. All three are efficient and well tolerated virus black muslim in the white house purchase ivermectin 3 mg online, and with all three, advantages take 4 to 6 weeks to develop. The underlying mechanism has not been established, but could contain inhibiting reuptake of serotonin, making extra of the transmitter obtainable for motion. Like different tricyclic antidepressants, amitriptyline could cause hypotension and anticholinergic results (dry mouth, constipation, urinary retention, blurred imaginative and prescient, tachycardia). Riboflavin (vitamin B2) can reduce the quantity and severity of migraine assaults, but benefits are modest and develop slowly. In two research, daily therapy with coenzyme Q-10 (CoQ-10) produced a big discount within the occurrence of migraine attacks in comparison with placebo. After 3 months, the variety of days on which complications occurred declined by no much less than 50% in 61% and 47% of study members, respectively. However, though headache frequency declined, headache depth was not affected. Extracts produced from the foundation of Petasites hybridus, a plant whose widespread name is butterbur, can reduce the frequency of migraine assaults. In a double-blind, placebo-controlled trial, about 1 in 5 sufferers taking seventy five mg of extract twice daily experienced a 50% or larger discount in migraine frequency. However, butterbur root incorporates pyrrolizidine alkaloids, which, if not removed throughout processing, can cause liver damage and most cancers. In the study noted, the preparation employed, bought as Petadolex, was pyrrolizidine free. Estrogens and Triptans for Menstrually Associated Migraine Menstrually related migraine is outlined as migraine that routinely occurs inside 2 days of the onset of menses. An essential trigger is the decline in estrogen levels that precedes menstruation. For many women, menstrually related migraine can be prevented by taking estrogen dietary supplements, which compensate for the premenstrual estrogen drop. Topical preparations-estrogen gel and estrogen patches [eg, Climara, Estraderm]-work well. Dosing is done for 7 days each month, starting 2 days before the expected assault. For instance, frovatriptan, naratriptan, and zolmitriptan can reduce the frequency, intensity, and length of menstrually associated migraine. Dosing is finished for six days every month, starting 2 days earlier than the expected onset of menses. In addition, naproxen sodium at a dosage of 550 mg twice daily, given 6 days before to 7 days after menses, has demonstrated effectiveness within the prevention of migraine. It has since been decided that the studies accomplished on verapamil and nimodipine demonstrated low levels of proof to help their use in migraine prophylaxis. Each attack lasts quarter-hour to 2 hours and is characterized by extreme, throbbing, unilateral pain within the orbital-temporal area (ie, close to the eye). A typical cluster consists of one or two such assaults daily for 2 to 3 months. Along with headache, sufferers usually expertise lacrimation, conjunctival redness, nasal congestion, rhinorrhea, ptosis (drooping eyelid), and miosis (constriction of the pupil)-all on the same aspect as the headache. Effective agents embrace glucocorticoids (prednisone and dexamethasone), verapamil, and lithium. High-dose prednisone (40 to eighty mg/day) or dexamethasone (4 mg twice daily) acts rapidly, producing results in forty eight hours. However, as a result of long-term use of glucocorticoids carries severe risks (see Chapter 72), remedy ought to cease in 1 to 2 months. The drug is efficient, but can cause multiple adverse effects, and dosing is difficult. To guarantee therapeutic results and reduce toxicity, blood levels of lithium have to be monitored; the target vary is zero. With all of those medicine, prophylactic therapy ought to be limited to the cluster cycle, and then discontinued when the present cycle is over. If an attack occurs regardless of preventive remedy, it can be aborted with sumatriptan or oxygen. Inhaling 100% oxygen (7 to 10 L/min for 15 to 20 minutes) is also highly effective, and has just about no antagonistic results. In the past, ergot preparations (eg, intravenous dihydroergotamine, sublingual ergotamine) have been commonly used. However, their use right now is restricted, as fashionable trials are small in population and lack proof that these medicine work any higher at relieving cluster headaches than placebo. Treatment consists of 31 injections, made into muscle tissue of the scalp, neck, and upper back. Treatment is expensive and benefits are modest: On common, patients expertise about 2 fewer headache days a month. Headache is often related to scalp tingling and a way of tightness or pressure within the head and neck. Depressive symptoms (sleep disturbances, including early and frequent awakening) are often current. By definition, continual tension-type headaches happen 15 or extra days per 30 days for at least 6 months. For prophylaxis, amitriptyline [Elavil], a tricyclic antidepressant, is the drug of choice. Dosing at bedtime will assist relieve any depression-related sleep disturbances in addition to protecting towards headache. Amitriptyline can cause anticholinergic unwanted side effects (eg, dry mouth, constipation) and poses a risk of cardiotoxicity at high doses (see Chapter 32). Instruction should embody cognitive coping abilities and information on relaxation techniques (eg, massage, scorching baths, biofeedback, deep muscle relaxation). The objective of abortive remedy is to remove headache ache and related nausea and vomiting. The goal of prophylactic remedy is to scale back the incidence and depth of migraine assaults. There are two kinds of drugs for abortive therapy: nonspecific analgesics (aspirin-like drugs and opioids) and migraine-specific drugs (triptans and ergot alkaloids). Aspirin-like analgesics (eg, acetaminophen, aspirin, naproxen) are effective for abortive remedy of gentle to average migraine. Opioid analgesics (eg, butorphanol, meperidine) are reserved for extreme migraine that has not responded to different medicine. Triptans (eg, sumatriptan) are first-line drugs for abortive therapy of moderate to extreme migraine. All triptans can be found in oral formulations, which have a relatively gradual onset. Two triptans-sumatriptan and zolmitriptan-are out there in fast-acting formulations (either nasal spray, subQ injection, or both). Overdose with ergotamine can cause ergotism, a severe situation characterized by severe tissue ischemia secondary to generalized constriction of peripheral arteries.
References
- Dehvari N, da Silva Junior ED, Bengtsson T, et al: Mirabegron: potential off target effects and uses beyond the bladder, Br J Pharmacol 175(21):4072n 4082, 2018.
- Catella-Lawson F, Reilly MP, Kapoor SC, et al. Cyclooxygenase inhibitors and the antiplatelet effects of aspirin. N Engl J Med 2001;345(25):1809-17.
- Kirwan WO, Turnbull RB Jr, Fazio VW, Weakley FL. Pullthrough operation with delayed anastomosis for rectal cancer. Br J Surg 1978;65(10):695-98.
- Anon. (1979). Drugs for dysmenorrhea, The Medical Letter on Drugs and Therapeutics, 21, 81.
- Freeman ME, Kanyicska B, Lerant A, et al: Prolactin: structure, function, and regulation of secretion, Physiol Rev 80(4):1523n1631, 2000.