

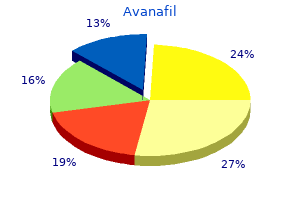
Avanafil
Bradley V. Vaughn, MD
- Professor of Neurology and Biomedical Engineering
- Vice-Chair, Department of Neurology
- Chief, Division of Sleep and Epilepsy
- University of North Carolina School of Medicine
- Chapel Hill, North Carolina
Avanafil dosages: 200 mg, 100 mg, 50 mg
Avanafil packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills
Avanafil 100 mg with mastercard
These allow for some extent of autonomous perform, in addition to transmitting results of central input impotence for erectile dysfunction causes generic avanafil 100 mg line. The dorsal vagal complex represents an important website the place the assorted influences that can alter gastric secretion are built-in impotence and high blood pressure discount avanafil 200 mg amex. Thus, the dorsal vagal advanced receives central input from the hypothalamus, in addition to visceral input from the nucleus tractus solitarius how does the erectile dysfunction pump work avanafil 100mg sale. There are many mechanisms, due to this fact, whereby the perform of the stomach is controlled. For instance, distension of the stomach wall prompts reflexes that stimulate acid secretion at the stage of the parietal cell. These may be quick reflexes, which contain neural transmission contained entirely inside the enteric nervous system. In addition, lengthy reflexes contain the activation of primary afferents that journey by way of the vagus nerve, which in flip are interpreted within the dorsal vagal complex and set off vagal outflow through efferent nerves that journey back to the stomach and activate parietal cells or different parts of the secretory machinery. At one time, histamine was regarded as the final common mediator of acid secretion, primarily based in part on the scientific remark that histamine H2 receptor antagonists can profoundly inhibit acid secretion. The physiological implication of this potentiation, or synergism, is that a higher stage of acid secretion can be produced with relatively small will increase in each of the three stimuli. The pharmacological significance is that merely interfering with the action of any certainly one of them can considerably inhibit acid secretion. In reality, synergism is a common theme in the management of several totally different features throughout the gastrointestinal system. Specifically, somatostatin is released from D cells in the antral mucosa when luminal pH decreases beneath three, and inhibits the release of gastrin from G cells. The example of pH is described earlier, but acid output, at least, is also elevated by parts of the meal. Short peptides and amino acids, derived from dietary protein, are capable of activating gastrin release from G cells. Stretch of the abdomen wall will increase acid secretion via each intrinsic reflexes and vagovagal reflexes. Gastrin launch is negatively regulated by luminal acidity via the release of somatostatin from antral D cells. However, as a end result of no meals is current, and thus no buffering capacity of the gastric contents, the low volume of secretions produced nonetheless has a low pH- normally around three. Gastrin secretion during the interdigestive interval, then again, is minimal. Cephalic Phase Even earlier than the meal is ingested, the abdomen is readied to obtain it by the cephalic. In reality, in the course of the cephalic phase, a quantity of gastrointestinal techniques in addition to the abdomen turn into activated, including the pancreas and gallbladder. Higher mind facilities respond to the sight, odor, taste, and even the considered food, and relay data to the dorsal vagal complicated. In turn, vagal outflow initiates both secretory and motor behavior in the abdomen and more distal segments. Gastric secretion occurring through the cephalic part readies the stomach to receive the meal. The intestinal phase of secretion could serve to ready the stomach for its subsequent meal. Gastric Phase the gastric phase of secretion is quantitatively the most important. In addition to vagal influences persevering with from the cephalic phase, secretion is now amplified additional by mechanical and chemical stimuli that arise from the presence of the meal in the lumen. These include the luminal signals discussed earlier, and signals arising from stretch receptors embedded in the wall of the stomach. The gastric part additionally involves modifications in motility and is accompanied by a marked enhance in gastric blood flow, which supplies the metabolic necessities of the actively secreting cell sorts. Moreover, pepsinogen launched by chief cells is rapidly cleaved to pepsin in an autocatalytic reaction that happens optimally at pH 2, and this pepsin then acts on ingested protein to launch short peptides and amino acids that further improve gastrin release. Moreover, many dietary substances, together with proteins, are extremely effective buffers. Thus, whereas acid secretory rates stay high, the efficient pH in the bulk of the lumen could improve to pH 5. The downstream targets of the signaling pathways linked to receptor occupancy are presumed to include cytoskeletal parts, ion channels, and the receptors themselves, the latter representing a mechanism of negative feedback. Cytoskeletal rearrangements are implied by the dramatic morphological modifications that happen as parietal cells transition from rest to secretion. At relaxation, the cytoplasm is full of the tubulovesicles and intracellular canaliculi. This enzyme generates protons and bicarbonate ions from the reaction of water and carbon dioxide. Protons are then pumped out of the cell throughout the apical membrane in exchange for potassium ions, with the consumption of mobile energy. They can due to this fact readily exit across the apical membrane via potassium channels which are additionally localized to the tubulovesicles, and that are opened when the parietal cell is stimulated. Specialized chloride channels are additionally current in this site, and serve to allow the apical exit of chloride ions to match the protons pumped from the cell. The general mechanism also wants to remind you of absorption of bicarbonate by the renal tubule, as was discussed in Chapter forty seven. Thus, as the protons are secreted apically, the parietal cells additionally discharge bicarbonate ions across the basolateral membrane to maintain up cytosolic pH within slender limits. At least a portion of this bicarbonate Intestinal Phase As contents move out of the abdomen into the duodenum, the buffering capacity of the lumen is reduced and the pH begins to decrease. At round pH 3, somatostatin release is triggered from D cells, and acts to suppress gastrin launch. Other indicators also restrict the extent of gastric secretion when the meal has moved into the small gut. For instance, the presence of fats within the small gut is related to a reduction in gastric secretion. Nevertheless, a portion of gastric secretion occurs as quickly as the meal is in the intestine. Bicarbonate ions are exported from the basolateral pole of the cell either by vesicular fusion or by way of a chloride/bicarbonate exchanger. Some bicarbonate is most likely going also lost secondary to pumping into intracellular vesicles (distinct from the tubulovesicles) that then move to the basolateral membrane and fuse with it, discharging their contents. The arrangement of the microvasculature in the gastric mucosa carries a portion of this bicarbonate as much as the basolateral pole of floor epithelial cells, which secrete bicarbonate to defend themselves towards the potentially injurious results of acid and pepsin.
Discount avanafil 50mg free shipping
The discharge of nociceptors increases with elevated drive and strain, however these functions range depending on probe dimension: the smaller the probe, the larger the response (Garell et al 1996) erectile dysfunction cause order avanafil 50mg amex. For cylindrical probes of different diameter, the discharges are comparable if the depth of the stimulus is calculated based on drive per length of the perimeter of the cylindrical probe erectile dysfunction in diabetic subjects in italy effective avanafil 100 mg. This suggests that the stress/strain most that happens on the edge of the cylindrical stimulus is the crucial parameter for excitation of nociceptor terminals erectile dysfunction drugs available over the counter discount 50 mg avanafil amex. For a given probe measurement, the response of A-fiber nociceptors will increase monotonically with pressure, whereas the response of C-fiber nociceptors becomes saturated at higher force levels. Mechanical stimuli had been presented to the receptive field of A-fiber and C-fiber nociceptors at completely different interstimulus intervals (with 10 minutes between stimulus pairs). The A-fiber response (triangles) recovered within 60 seconds, whereas the C-fiber response (circles) took more than a hundred and fifty seconds to get well. To normalize the information, the response to the test stimulus was divided by the response to the immediately preceding conditioning stimulus. However, the transducer components that account for mechanosensitivity are probably different from those responsible for warmth. A-fiber nociceptors seem like responsible for the sharp ache reported in response to punctate mechanical stimuli: (1) the reaction time to perception of pain is short, (2) the stimulus�response function of A-fiber nociceptors. Comparison of responses of nociceptors to mechanical stimuli in the monkey with pain ratings in human subjects. These knowledge provide proof that A-fiber nociceptors signal the pain reported from sharp probes. A, Average responses of A-fiber nociceptors (triangles) and C-fiber nociceptors (circles) to controlled-force stimuli. The A fibers exhibited a monotonically rising response, whereas the response of the C fibers reached a plateau at the higher force levels (0. B, Average pain ratings in response to controlled-force stimuli (open circle) increased monotonically in a manner similar to that noticed for the A-fiber nociceptors. Selective block of A-fiber function led to a major lower in ache ratings (filled circles). Klement and Arndt (1992) demonstrated that chilly ache could presumably be evoked by chilly stimuli utilized within the veins of human topics. A local anesthetic applied within the vein, but not within the overlying skin, abolished cold ache sensibility. It is subsequently possible that chilly pain is served, no less than in part, by vascular receptors. Just as the feeling of warmth is served by a specific set of major afferents (predominantly C fibers), the sense of cooling is served by a specific set of major afferents. They exhibit ongoing exercise at room temperature, and their response will increase markedly with mild cooling. Although the overwhelming majority of nociceptors have some response to ice stimuli applied to the skin, Simone and Kajander (1997) showed that all A-fiber nociceptors reply to cold stimuli beneath 0�C. C-fiber nociceptors may play a task in signaling chilly pain sensation as well (LaMotte and Thalhammer 1982). This channel is present in a subset of nociceptive sensory neurons which are conscious of intense warmth and capsaicin. There is, in reality, a dynamic plasticity that relates stimulus depth and sensation. Hyperalgesia is outlined as a leftward shift of the stimulus� response operate that relates the magnitude of ache to stimulus depth. It is evident that the edge for pain is lowered and pain in response to suprathreshold stimuli is enhanced. Hyperalgesia is a consistent function of somatic and visceral tissue harm and irritation. Pharyngitis is related to hyperalgesia in pharyngeal tissues such that merely swallowing induces pain. Micturition in the presence of a urinary tract an infection is painful, again reflecting the presence of hyperalgesia. The peripheral neural mechanisms of hyperalgesia have been studied in various tissues, together with the joints, cornea, testicle, gastrointestinal tract, and bladder. Hyperalgesia occurs not solely at the web site of injury but also within the surrounding unhurt space. Hyperalgesia at the website of damage is termed primary hyperalgesia, whereas hyperalgesia in the uninjured skin surrounding the harm is termed secondary hyperalgesia (Lewis 1935). For instance, it will be shown that nociceptors will become sensitized to mechanical stimuli (the power type of the test stimulus), but only after certain forms of harm. An experimental design incessantly used for study of the neural mechanisms of hyperalgesia is to characterize the response properties of a given fiber, then apply a manipulation that under ordinary circumstances would produce hyperalgesia, and eventually assess whether this manipulation has altered the response properties of the fiber in query. Cutaneous hyperalgesia has been studied after thermal injury (burn or freeze lesions), after local administration of chemical substances. The primary options of the hyperalgesia that develops after these varied accidents are quite comparable. In many instances the ache from these agents probably results from tissue damage and is subsequently indirect. Intradermal injection of capsaicin produces intense burning ache that lasts for several minutes. Another chemical of interest is histamine, which produces a long-lasting itch when applied to the skin. Histamine probably prompts nociceptors via the H1 receptor located on peripheral terminals. In about half of regular subjects, cowhage-induced itch is greatly attenuated during 12 Section One Neurobiology of Pain A eight. Responses to warmth stimuli had been obtained 5 minutes earlier than and 10 minutes after a 53�C, 30-second burn on the glabrous skin of the hand. Thus, peripheral neural mechanisms are prone to account for at least some features of primary hyperalgesia. The hyperalgesia is manifested as a leftward shift of the stimulus�response perform that relates the magnitude of ache to stimulus intensity. For instance, the 41�C stimulus was not painful before the burn however after the injury was as painful because the 49�C stimulus earlier than the damage. Peripheral Sensitization as a Mechanism for Primary Hyperalgesia to Heat Stimuli Substantial proof favors the idea that the first hyperalgesia to warmth stimuli that develops on the website of a burn injury is mediated by sensitization of nociceptors (Meyer and Campbell 1981a, LaMotte et al 1982). Sensitization is defined as a leftward shift of the stimulus�response function that relates the magnitude of the neural response to stimulus intensity. Sensitization is characterized by a decrease in threshold, an augmented response to suprathreshold stimuli, and ongoing spontaneous exercise. Experimental configurations for testing the neural mechanisms of major and secondary hyperalgesia. To examine secondary hyperalgesia, the site of injury and the positioning of testing should not coincide (C and D). Example of sensitization to mechanical stimuli for an A-fiber nociceptor following a chemical injection. C, Sensitization to mechanical stimuli was demonstrated in this fiber half-hour after chemical injection.

Order avanafil 100 mg otc
Knowledge that a vein have to be current at this website, even when not visible in an obese or collapsed patient, could also be life-saving when pressing transfusion is required erectile dysfunction over 65 avanafil 200 mg amex. Occasionally, the instantly adjoining saphenous nerve is caught up by a ligature during this process � the affected person, if aware, will complain bitterly of pain if this is done erectile dysfunction houston buy 50 mg avanafil fast delivery. Usually that is idiopathic however could outcome from the increased venous strain caused by more proximal venous obstruction (a pelvic tumour or the pregnant uterus, for example) or could also be secondary to obstruction of the deep venous pathway of the leg by thrombosis popular erectile dysfunction drugs 50 mg avanafil with amex. This is especially liable to occur over the subcutaneous anteromedial surface of the tibia where the cutaneous blood provide is least generous. The proximal termination of the great saphenous vein at the groin is found by palpating the femoral pulse. The nice saphenous vein is distinguished from the femoral vein in that (a) it lies in the superficial fascia, whereas the femoral vein lies deep to the deep facia, and (b) the great saphenous vein bears numerous tributaries, whereas the femoral vein receives only the nice saphenous vein. There is basically no excuse for the occasional disaster of the femoral vein being injured in varicose vein surgical procedure. There are two exceptions: the obturator nerve appears at the medial border of psoas tendon, and the genitofemoral nerve emerges on the anterior facet of the muscle. The principal branches of the plexus are the femoral nerve and the obturator nerve. Its branches are: � muscular � to the anterior compartment of the thigh (quadriceps, sartorius and pectineus); T12 L1 Subcostal nerve Iliohypogastric nerve Ilio-inguinal nerve Genitofemoral nerve L3 Lateral cutaneous nerve of thigh L4 Contribution to lumbosacral trunk Femoral nerve L2 Obturator nerve. The course and distribution of the principal nerves 273 � cutaneous � the medial and intermediate cutaneous nerves of the thigh and the saphenous nerve, which traverses the adductor canal to supply the pores and skin of the medial aspect of the leg, ankle and foot to the nice toe; � articular � to the hip and knee joints. The femoral nerve provides the pores and skin of the medial and anterior aspects of the thigh by way of its medial and intermediate cutaneous branches, but the lateral aspect is supplied by the lateral cutaneous nerve of the thigh (L2�L3). This arises instantly from the lumbar plexus and enters the thigh often by passing deep to the inguinal ligament. Occasionally, the nerve pierces the ligament and should then be pressed upon by it with resultant ache and anaesthesia over the higher outer thigh (meralgia paraesthetica). This is relieved by dividing the deeper fasciculus of the inguinal ligament where the nerve passes over it. The obturator nerve (L2�L4) emerges from the medial aspect of the psoas and runs downwards and forwards, deep to the inner iliac vessels, to achieve the superior part of the obturator foramen. This the nerve traverses, in company with the obturator vessels, to enter the thigh. Its branches are: � muscular � to obturator externus, the adductor muscle tissue and gracilis; � cutaneous � to an area of skin over the medial facet of the thigh; � articular � to the hip and knee joints. This could be performed through a midline lower abdominal incision exposing the nerve trunk extraperitoneally on both sides because it passes towards the obturator foramen. Pressure of a strangulated obturator hernia upon the nerve causes referred pain in its area of cutaneous distribution, in order that intestinal obstruction related to ache along the medial facet of the thigh ought to suggest this diagnosis. Note that L4 is shared by both plexuses, a department from it joining L5 to type the lumbosacral trunk, which carries its essential contribution to the sacral plexus. Branches from the plexus supply: � the pelvic muscular tissues; � the muscles of the hip; � the skin of the buttock and the again of the thigh. It has a fancy course, passing from the pelvis, briefly through the gluteal region, along the side-wall of the ischiorectal fossa and through the deep perineal pouch to end by supplying the skin of the external genitalia. It crosses the dorsum of the ischial spine and immediately disappears via the lesser sciatic foramen into the perineum. Within the canal it first offers off the inferior rectal nerve, which crosses the fossa the course and distribution of the principal nerves 275 Gluteus maximus (cut) Superior gluteal artery and nerve Gluteus medius Piriformis Inferior gluteal nerve, artery and vein Internal pudendal artery and nerve Posterior cutaneous nerve of thigh Sciatic nerve (a) Obturator internus and gemelli Greater trochanter Quadratus femoris Bony and ligamentous framework Greater sciatic foramen Sacrotuberous ligament Ischial spine Sacrospinous ligament Lesser sciatic foramen (b). It bifurcates nearly at once; its deeper branch supplies the sphincter urethrae and the opposite muscle tissue of the anterior perineum (the ischiocavernosus, bulbospongiosus and the superficial and deep transverse perinei). Its extra superficial branch innervates the skin of the posterior facet of the scrotum or vulva. The dorsal nerve of the penis (or clitoris) traverses the deep perineal pouch, pierces the perineal membrane and then penetrates the suspensory ligament of the penis to provide the dorsal facet of this construction. Alternatively, the needle could be launched simply medial to the ischial tuberosity to a depth of 1 in (2. The sciatic nerve the sciatic nerve (L4, L5, S1�S3) is the biggest nerve within the physique. Note that gluteus medius has been eliminated to show the otherwise completely hidden gluteus minimus. Here, it lies deep to the hamstrings and is crossed only by the lengthy head of biceps. The sciatic nerve terminates by dividing into the tibial and common peroneal nerves. Branches the trunk of the sciatic nerve provides the hamstring muscular tissues (biceps, semimembranosus, semitendinosus) and also the adductor magnus, the latter being innervated additionally by the obturator nerve. All the muscle branches apart from the one to the short head of biceps come up on the medial side of the nerve; its lateral border is therefore the facet of relative safety in its operative exposure. Sensory loss is complete under the knee, aside from an area along the medial aspect of the leg, over the medial malleolus and all the method down to the hallux, which is innervated by the saphenous branch of the femoral nerve. The artery have to be neatly isolated and tied without any nerve fibres being included within the ligature, since this is in a position to be followed by severe ache in the stump. It then descends deep to soleus, in firm with the posterior tibial vessels, passes on their lateral side behind the medial malleolus to end by dividing into the medial and lateral plantar nerves. Its terminal plantar branches provide the intrinsic muscular tissues and skin of the sole of the foot; the medial plantar nerve having an equal distribution to that of the median nerve within the hand, the lateral plantar nerve being corresponding to the ulnar nerve. The widespread peroneal (fibular) nerve the widespread peroneal nerve (L4, L5, S1, S2) is the smaller of the terminal branches of the sciatic nerve. It enters the upper part of the popliteal fossa, passes along the medial border of the biceps tendon, then curves across the neck of the fibula the place it lies within the substance of peroneus longus and divides into its terminal branches, the deep peroneal and superficial peroneal nerves. Branches While still in the popliteal fossa, the widespread peroneal nerve provides off the lateral cutaneous nerve of the calf, a peroneal (sural) communicating department and twigs to the knee joint, but has no muscular branches. The deep peroneal (fibular) nerve the deep peroneal nerve pierces extensor digitorum longus, then descends, in company with the anterior tibial vessels, over the interosseous membrane and then over the ankle joint. Medially lies tibialis anterior, whereas laterally lies first extensor digitorum longus, then extensor hallucis longus. Its branches are: � muscular � to the muscular tissues of the anterior compartment of the leg � extensor digitorum longus, extensor hallucis longus, tibialis anterior, peroneus tertius � and extensor digitorum brevis; � cutaneous � to a small area of skin in the net between the 1st and 2nd toes. Compartments of the lower limb 279 the superficial peroneal (fibular) nerve the superficial peroneal nerve runs within the lateral compartment of the leg. Its branches are: � muscular � to the lateral compartment muscular tissues (peroneus longus and brevis); � cutaneous � to the skin of the distal two-thirds of the lateral facet of the leg and to the dorsum of the foot (apart from the small area between the first and 2nd toes provided by the deep peroneal nerve). It may be damaged at this site by the stress of a decent bandage or plaster forged or may be torn in severe adduction accidents to the knee.
Purchase avanafil 100mg with visa
Monoclonal proteins have been proven to be answerable for lupus anticoagulants,196,197 acquired protein S deficiency,198,199 acquired activated protein C resistance,200 and inhibition of tissue plasminogen activator impotence and alcohol buy generic avanafil 100mg on-line. Most sufferers become symptomatic when the serum viscosity is 6 or 7 centipoise (normal is less than or equal to 1 impotence essential oils avanafil 50 mg without prescription. Evidence of acute and continual pyelonephritis were observed in 20% and 23% of circumstances, respectively erectile dysfunction early age generic avanafil 50 mg. Plasma cell infiltrates and amyloid could also be noticed in 10% and 5% of instances, respectively. They defined the syndrome as rapidly progressive illness with an unexplained fever and pancytopenia and a hypercellular marrow. Other much less frequent areas of myelomatous involvement were the lung, pleura, adrenal glands, pancreas, and testis. Once the choice has been made to treat for symptomatic illness, a longterm plan for managing the illness ought to be formulated before instituting remedy. Third, concurrent corticosteroid therapy, both as part of the regimen or for other indications, may confound interpretation of efficacy. In the earliest literature, response included such factors as rising hemoglobin concentration or efficiency standing, or decreasing blood urea nitrogen ranges. It was not till the appearance of high-dose melphalan that investigators227,228 began to define an entire remission category. Subsequent definitions have required immunofixation negativity to qualify as complete remission. Cyclophosphamide has mostly been utilized in multidrug combinations for induction, for therapy in relapse, and for stem cell mobilization rather than as a single agent for induction, as has melphalan. Surprisingly, Mass240 failed to indicate a distinction between the survival of 55 sufferers randomly assigned to prednisone therapy or placebo regardless of medical improvement within the former group. Subsequently, high-dose corticosteroids have been proven to supply response charges of 40% to 50% in previously untreated sufferers, and 25% Cyclophosphamide Korst et al. Authors observe that much quicker response observed with prednisone but worse survival with prednisone in poor-risk sufferers. Patients had been started on 200 mg every evening; the dose was escalated every 2 weeks, if tolerated, to a ultimate maximal dose of 800 mg daily. A complete of 25% of patients had at least a 50% reduction in their serum paraprotein. Preliminary evidence of response was obvious within 2 months in additional than three quarters of the patients who did respond. There can additionally be an increased danger of thrombosis in sufferers handled with thalidomide, which seems to be exacerbated by method of concurrent mixture chemotherapy, with charges as excessive as 28%. Its activity as a single agent in relapsed or refractory illness is modest, with response charges of about 10%. Response rates of 0% to 27% have been observed in relapsed and refractory sufferers with single-agent oral regimens (30 mg/week in three divided doses given three of 5 weeks or forty mg/m2 each 3 weeks). In addition, there are two anecdotal reports of activity of low-dose (25 to 50 mg/day) oral etoposide. Bendamustine Bendamustine is a multifunctional alkylating agent with a purinelike ring system and a novel mechanism of motion. Bendamustine 100 mg/m2 on days 1 and a pair of per cycle was discovered to be the maximal tolerated dose. The general response price was 55% with a median progression-free survival of 26 (0 to 61) weeks. In vitro research even have shown potent inhibitory effect on osteoclast differentiation in addition to bone marrow angiogenesis. Additional studies have been accomplished as are described within the section of relapsed/refractory illness. In bortezomib-na�ve sufferers,221 reponse charges had been seen in 25% of sufferers handled at the 20 mg/m2 stage and in 52% of patients handled with first cycle 20 mg/m2, however subsequent cycles at 27 mg/m2. The commonest unwanted side effects of drug are fatigue, nausea, anemia, dyspnea, cough, and pyrexia occurring in 34% to 62% of patients. Because fever, chills, shortness of breath, and/or rigors might occur during cycle 1 and sometimes cycle 2, dexamethasone 4 mg every day can be given earlier than each dose in cycle 1 and before the first dose of the cycle 2 if dose escalation is deliberate. It is a boronic acid dipeptide that reversibly and selectively inhibits the proteasome, an intracellular complex that degrades primarily ubiquitinated proteins. The proteasome has a key function in protein degradation, cell-cycle regulation, and gene expression. Inhibition of the proteasome has emerged as an necessary antitumor target, and bortezomib has been shown in vitro and in vivo to cause progress arrest, to induce apoptosis, and to inhibit angiogenesis. There were 75% of sufferers who had severe (grade three to 4) opposed events, the most typical of which have been thrombocytopenia, neutropenia, anemia, gastrointestinal disturbances, fatigue, and peripheral neuropathy (sensory, motor, and pain). Grade 3 neuropathy was more likely to occur in sufferers with a baseline neuropathy. A whole of 71% of patients with neuropathy larger than or equal to grade 3 and/or requiring discontinuation who had decision to baseline or improvement. Subcutaneous administration and/or weekly administration of bortezomib reduces the incidence of extreme peripheral neuropathy by practically 40%. Because of toxicity, two important modifications to bortezomib administration have been revamped the previous decade. The first was introduction of weekly bortezomib rather than twice weekly followed by a 10-day rest; the second was the subcutaneous administration somewhat than the intravenous route of administration. A total of 14 sufferers were treated with 10 mg/m2 for 7 days by steady infusion, and a couple of responded. The drug has been incorporated into other regimens for relapsed disease274,327,328 and induction therapy. Topotecan induces significant toxicity together with greater than or equal to grade 3 granulocytopenia and thrombocytopenia in 93% and 53% of sufferers, respectively. Agents within the former category embrace diamidines, such as stilbamidine; 1-aminocyclopentanecarboxylic acid; amsacrine, 339,340 aclarubin,341 chlorozotocin,342 hexamethylmelamine343 and azaserine. The total response fee was 91%, with 6% achieving full response and 32% superb partial response. A whole of 47% of patients skilled grade three or larger nonhematologic toxicity, mostly fatigue (15%). The rationale for the clarithromycin use is that it alters the hepatic metabolism of each medication, resulting in higher effective doses. The lenalidomide schedule was as above, but dexamethasone was administered solely as soon as weekly. Because of the ease of administration and low early dying price, many consider Rd an excellent first-line therapeutic option. Due to high rates of neuropathy, recommended modification is to begin with weekly administration and 5-week cycles. Rates of other secondary main malignancies have been comparable in each arms and inside the expected vary for an elderly inhabitants. The overall response fee was 88%, with 39% attaining complete/near full response. A modified extension of that trial included another 30 sufferers to maximize dose delivery and scale back toxicity.
Cheap avanafil 50 mg on-line
At the tibia Compare the space from the line of the knee joint to the medial malleolus on both sides impotence organic origin definition avanafil 200mg otc. Muscles and tendons Quadriceps femoris types the distinguished muscle mass on the anterior facet of the thigh; its insertion into the medial facet of the patella could be seen to extend extra distally than on the lateral aspect erectile dysfunction treatment levitra purchase 200mg avanafil fast delivery. In the well-developed subject, sartorius may be defined when the hip is flexed and externally rotated in opposition to resistance impotent rage violet cheap 100 mg avanafil with amex. It extends from the anterior superior iliac spine to the medial side of the upper end of the tibia and, as the lateral border of the femoral triangle, it is an important landmark. Gluteus maximus types the majority of the buttock and may be felt to contract in extension of the hip. Gluteus medius and minimus and the adductors can be felt to tighten, respectively, in resisted abduction and adduction of the hip. Between the tendons of biceps and semitendinosus could be felt the heads of origin of gastrocnemius. This muscle, with soleus, varieties the bulk of the posterior bulge of the calf; the 2 end distally within the Achilles tendon (calcaneal tendon). More laterally, the tendons of extensor hallucis longus and extensor digitorum longus are readily seen within the dorsiflexed foot. Behind the medial malleolus, from the medial to the lateral aspect, cross the tendons of tibialis posterior and flexor digitorum longus, the posterior tibial artery with its venae comitantes, the tibial nerve and, finally, flexor hallucis longus. The higher two-thirds of a line becoming a member of this level to the adductor tubercle, with the hip somewhat flexed, abducted and externally rotated, accurately defines the floor marking of this vessel. The pulse is sought by firm pressure downwards in opposition to the popliteal fossa of the femur. In approximately 1% of healthy topics this artery is replaced by the peroneal (fibular) artery. The small (or short) saphenous vein commences as a continuation of the veins on the lateral facet of the dorsum of the foot, runs proximally behind the lateral malleolus, and terminates by draining into the popliteal vein behind the knee. The nice (or long) saphenous vein arises from the medial the floor anatomy and surface markings of the decrease limb 231 Peroneus brevis Anterior tibial artery Perforating branch of peroneal artery Superior and inferior extensor retinacula Dorsalis pedis artery Extensor digitorum longus and brevis Tibialis anterior Extensor hallucis longus Extensor digitorum brevis slip to hallux Peroneus tertius. These veins are readily studied in any affected person with in depth varicose veins and are usually seen, in their lower part, within the skinny regular topic on standing. Anterior superior iliac backbone Inguinal ligament Midline Femoral artery Adductor hiatus in adductor magnus Popliteal artery Adductor tubercle. The floor anatomy and surface markings of the lower limb 233 Great saphenous vein Medial malleolus. From the practical perspective, the position of the long saphenous vein immediately in front of the medial malleolus is probably the most important single anatomical relationship; no matter how collapsed or obese, or how young and tiny the patient, the vein can be relied upon to be obtainable at this site when urgently required for transfusion purposes. Nerves Only one nerve is definitely felt in the lower limb; this is the frequent peroneal (fibular) nerve, which may be rolled in opposition to the bone as it winds around the neck of the fibula. Not unnaturally, it may be injured at this web site in adduction accidents to the knee or compressed by a decent plaster cast or firm bandage, with a resultant foot drop and inversion (talipes equinovarus; see web page 279). After a course of roughly 2 in (5 cm) the nerve breaks up into its terminal branches. The nerve ends at a variable level above the popliteal fossa by dividing into the tibial and common peroneal nerves, respectively. It would appear inconceivable that a nerve with such fixed and welldefined landmarks could probably be broken by intramuscular injections, but this has happened so regularly that it has critically been proposed that this site must be prohibited. The normal recommendation is to make use of the upper outer quadrant of the buttock 234 the lower limb. Join the midpoint between the ischial tuberosity and posterior superior iliac backbone to the midpoint between the ischial tuberosity and the higher trochanter by a curved line; continue this line vertically down the leg � it represents the course of the sciatic nerve. Many health-care professionals, however, have an entirely completely different mental image of the buttock; a much smaller and extra aesthetic affair comprising merely the hillock of the natus. An injection into the higher outer quadrant of this diminutive structure lies in the instant vicinityof the sciatic nerve! Sciatic nerve thumb and thenar eminence are placed along the iliac crest with the tip of the thumb touching the anterior superior iliac backbone. It is 18 in (45 cm) in size, a measurement it shares with the vas, the spinal cord and the thoracic duct and which can be the space from the enamel to the cardia of the stomach. The femoral head is two-thirds of a sphere and faces upwards, medially and forwards. It is roofed with articular hyaline cartilage apart from its central fovea, where the ligamentum teres is hooked up. The junction between the neck and the shaft is marked anteriorly by the trochanteric line, laterally by the larger trochanter, medially and considerably posteriorly by the lesser trochanter and posteriorly by the distinguished trochanteric crest, which unites the 2 trochanters. The blood supply to the femoral head is derived from vessels travelling up from the diaphysis along the cancellous bone, from vessels in the hip capsule, the place this is mirrored onto the neck in longitudinal bands or retinacula, and from the artery in the ligamentum teres; this third supply is negligible in adults, but essential in youngsters, when the femoral head is separated from the neck by the cartilage of the epiphyseal line. The femoral shaft is roughly circular in part at its center but is flattened posteriorly at each extremity. Inferiorly, this crest splits into the medial and lateral supracondylar lines, leaving a flat popliteal floor between them. The decrease finish of the femur bears the outstanding condyles, that are separated by a deep intercondylar notch (fossa) posteriorly but which mix anteriorly to form an articular surface for the patella. The lateral condyle is the more distinguished of the two and acts as a buttress to assist in stopping lateral displacement of the patella. The bones and joints of the decrease limb 237 Iliac crest Posterior superior backbone Greater sciatic notch Ischial spine Lesser sciatic notch Ischial tuberosity Lesser trochanter Spiral line Greater trochanter Intertrochanteric crest Gluteal crest Pectineal line Linea aspera. The neck might break immediately beneath the top (subcapital), close to its midpoint (cervical) or adjoining to the trochanters (basal), or the fracture line might pass between, along or just beneath the trochanters. Fractures of the femoral neck will interrupt completely the blood supply from the diaphysis and, ought to the retinacula also be torn, avascular necrosis of the head shall be inevitable. There is a curious age sample of hip accidents: kids may maintain greenstick fractures of the femoral neck; schoolboys might displace the epiphysis of the femoral head; in grownup life the hip dislocates; and in old age fracture of the neck of the femur again turns into the similar old lesion. The proximal segment is flexed by iliacus and psoas and abducted by gluteus medius and minimus, whereas the distal segment is pulled medially by the adductor muscles. Reduction requires powerful traction, to beat the shortening, and then manipulation of the distal fragment into line with the proximal section; the limb should subsequently be abducted and in addition pushed forwards through the use of a large pad behind the knee. Fractures of the decrease end of the shaft, immediately above the condyles, are relatively rare; fortuitously so, as a result of they are often extraordinarily tough to treat for the reason that small distal fragment is tilted backwards by gastrocnemius, the only muscle which is connected to it. The sharp proximal fringe of this distal fragment may tear the popliteal artery, which lies instantly behind it. This may outcome from adduction fractures, slipped femoral epiphysis or bone-softening ailments. Coxa valga, during which the angle is elevated, is much rarer but happens in impacted abduction fractures. Note, nonetheless, that in kids the traditional angle between the neck and shaft is approximately 160�. The posterior surface of the patella is covered with cartilage and articulates with the 2 femoral condyles by means of a larger lateral and smaller medial aspect. The patella may be fractured transversely by violent contraction of the quadriceps � for example, in trying to stop a backwards fall. In this case, the tear extends outwards into the quadriceps expansion, permitting the higher bone fragment to be pulled proximally; there may be (b) Vastus medialis (a).
Generic 50mg avanafil otc
The hydration of carbon dioxide leads to the formation of carbonic acid, which then can dissociate right into a hydrogen ion and a bicarbonate ion, as discussed in Chapter 36 erectile dysfunction doctors in texas 200 mg avanafil for sale. Conversely, for any particular pH and Pco2, only one bicarbonate ion concentration will satisfy the Henderson�Hasselbalch equation erectile dysfunction topical treatment purchase 100 mg avanafil visa. If the Pco2 is held constant, for example, at forty mm Hg, an isobar line could be constructed, connecting the resulting points because the pH is various erectile dysfunction gabapentin cheap 200 mg avanafil with mastercard. If every little thing else stays fixed, hypoventilation leads to acidosis; hyperventilation leads to alkalosis. The buffer value of plasma within the presence of hemoglobin is 4 to 5 occasions that of plasma separated from erythrocytes. Although a quantity of potential buffering groups are discovered on proteins, just one large group has pK in the pH vary encountered in the blood. Thus, as oxygen leaves hemoglobin within the tissue capillaries, the imidazole group removes hydrogen ions from the erythrocyte interior, permitting more carbon dioxide to be transported as bicarbonate. The bicarbonate buffer system is the most important buffer found within the interstitial fluid, together with the lymph. The volume of the interstitial compartment is much bigger than that of the plasma, so the interstitial fluid might play an necessary function in buffering. The extracellular portion of bone accommodates very large deposits of calcium and phosphate salts, mainly in the type of hydroxyapatite. In an otherwise healthy grownup, where bone growth and resorption are in a steady state, bone salts can buffer hydrogen ions in persistent acidosis. Chronic buffering of hydrogen ions by the bone salts may due to this fact result in demineralization of bone. The intracellular proteins and natural phosphates of most cells can operate to buffer each fastened acids and carbonic acid. These primary acid�base issues could occur singly ("easy") or together ("blended") or may be altered by compensatory mechanisms. Sensors uncovered to the arterial blood and to the cerebrospinal fluid present the central controllers of respiration with the knowledge needed to regulate the arterial Pco2 at or close to forty mm Hg (see Chapter 38). The pHa at any Paco2 is decided by the bicarbonate and other buffers current within the blood. As shown in Table 37�2, despair of the respiratory centers in the medulla (see Chapter 38) by anesthetic agents, narcotics, hypoxia, central nervous system illness or trauma, and even tremendously increased PaCo2 itself leads to hypoventilation and respiratory acidosis. Depression of the respiratory control facilities Anesthetics Sedatives Opiates Brain damage or disease Severe hypercapnia, hypoxia Neuromuscular issues Spinal wire harm Phrenic nerve harm Poliomyelitis, Guillain�Barr� syndrome, etc. Botulism, tetanus Myasthenia gravis Administration of curarelike drugs Diseases affecting the respiratory muscles Chest wall restriction Kyphoscoliosis Extreme obesity Lung restriction Pulmonary fibrosis Sarcoidosis Pneumothorax, pleural effusions, and so on. Restrictive, obstructive, and obliterative ailments of the lungs can also lead to respiratory acidosis. The decreased Paco2 shifts the equilibrium of the series of reactions describing carbon dioxide hydration and carbonic acid dissociation to the left. This leads to a decreased arterial hydrogen ion concentration, elevated pH, and a decreased plasma bicarbonate focus. As proven in Table 37�3, hyperventilation syndrome, a psychological dysfunction of unknown trigger, results in continual or recurrent episodes of hyperventilation and respiratory alkalosis. Drugs, hormones (such as progesterone), toxic substances, central nervous system diseases or problems, 25 20 15 10 7. Ingested drugs or toxic substances Methanol Ethanol Salicylates Ethylene glycol Ammonium chloride Loss of bicarbonate ions Diarrhea Pancreatic fistulas Renal dysfunction Lactic acidosis Hypoxemia Anemia, carbon monoxide Shock (hypovolemic, cardiogenic, septic, and so on. It may be attributable to the ingestion, infusion, or production of a fixed acid; decreased renal excretion of hydrogen ions; the movement of hydrogen ions from the intracellular to the extracellular compartment; or the loss of bicarbonate or other bases from the extracellular compartment. As shown in Table 37�4, ingestion of methyl alcohol or salicylates can cause metabolic acidosis by growing the fastened acids in the blood. Renal dysfunction can result in an inability to excrete hydrogen ions, in addition to an incapability to reabsorb bicarbonate ions, as will be discussed within the subsequent section. True "metabolic" acidosis could additionally be attributable to an accumulation of lactic acid in severe hypoxemia or shock and by diabetic ketoacidosis. Pco2 is unchanged, hydrogen ion concentration is decreased, and the ratio of bicarbonate focus to carbon dioxide is increased. As shown in Table 37�5, loss of gastric juice by vomiting results in a loss of hydrogen ions and will cause metabolic alkalosis. Loss of hydrogen ions Vomiting Gastric fistulas Diuretic therapy Treatment with or overproduction of steroids (aldosterone or other mineralocorticoids) Ingestion or administration of extra bicarbonate or other bases Intravenous bicarbonate Ingestion of bicarbonate or different bases. Compensation for acidosis or alkalosis in these circumstances should subsequently come from outside the respiratory system. The respiratory compensatory mechanism can operate very rapidly (within minutes) to partially right metabolic acidosis or alkalosis. The two major compensatory mechanisms are functions of the respiratory and renal systems. They can even compensate for respiratory alkalosis or metabolic alkalosis of nonrenal origin by decreasing hydrogen ion excretion and by decreasing the retention of filtered bicarbonate. Renal compensatory mechanisms for acid�base disturbances operate much more slowly than respiratory compensatory mechanisms. For example, the renal compensatory responses to sustained respiratory acidosis or alkalosis may take 3�6 days. The kidneys assist regulate acid�base steadiness by altering the excretion of fixed acids and the retention of the filtered bicarbonate; the respiratory system helps regulate physique acid�base stability by adjusting alveolar ventilation to change alveolar Pco2. As mentioned in Chapter 33, if carbon dioxide manufacturing is constant, the alveolar Pco2 is inversely proportional to the alveolar ventilation. In metabolic acidosis, the elevated blood hydrogen ion concentration stimulates chemoreceptors, which, in flip, increase alveolar ventilation, thus lowering arterial Pco2. As the respiratory compensation for the metabolic acidosis occurs, in the type of an increase in air flow, the arterial Pco2 decreases. The point representing blood pHa, Paco2, and bicarbonate concentration would then transfer a short distance along the lower-than-normal buffer line (from level G toward point H) till a brand new decrease Paco2 is attained. The respiratory compensation for metabolic acidosis occurs almost simultaneously with the event of the acidosis. The respiratory compensation for metabolic alkalosis is to lower alveolar ventilation, thus rising Paco2. Point D represents uncompensated metabolic alkalosis; respiratory compensation would transfer the blood pHa, PaCo2, and bicarbonate concentration point a brief distance along the new higher-than-normal blood�buffer line towards point F. Again the compensation happens because the alkalosis develops, with the point transferring along an intermediate course. The plasma bicarbonate can then be calculated from the pH and Pco2 by utilizing the Henderson�Hasselbalch equation. This could be done instantly, or by using a nomogram, or by graphical evaluation such because the pH�bicarbonate diagram (the "Davenport plot," after its popularizer), the pH� Pco2 diagram (the "Siggaard-Andersen"), or the composite acid�base diagram. Table 37�6 summarizes the changes in pHa, Paco2, and plasma bicarbonate focus that happen in easy, blended, and partially compensated acid�base disturbances. A easy method to decoding a blood fuel set is to first have a glance at the pH to determine whether or not the predominant problem is acidosis or alkalosis.
Order avanafil 100 mg
Whatever causes the hysteresis seems to be associated to surface rigidity within the lung diabetes-induced erectile dysfunction epidemiology pathophysiology and management buy cheap avanafil 100mg. The curve at left (saline inflation) subsequently represents the elastic recoil as a end result of solely the lung tissue itself; the curve at proper demonstrates the recoil because of each the lung tissue and the floor tension forces erectile dysfunction for young adults buy avanafil 100 mg on line. The distinction between the two curves is the recoil due to floor pressure forces testosterone associations with erectile dysfunction diabetes and the metabolic syndrome avanafil 50mg online. The demonstration of the big role of floor rigidity forces in the recoil strain of the lung led to consideration of how floor pressure affects the alveoli. If surface pressure is independent of surface area, the smaller the alveolus on the proper becomes, the higher the stress in it. Thus, if the lung had been composed of interconnected alveoli of different sizes (which it is) with a constant surface tension at the air�liquid interface, it might be inherently unstable, with an inclination for smaller alveoli to collapse into larger ones. This is usually not the case, which is fortunate because collapsed alveoli require very great distending pressures to reopen, partly because of the cohesive forces at the liquid�liquid interface of collapsed alveoli. At least two components cause the alveoli to be more secure than this prediction primarily based on constant floor T P1 r T P2 2r (3) P1 T r P2 T 2r (4) where this the wall pressure, P the stress contained in the alveolus, and r the radius of the alveolus. The surface pressure of most liquids (such as water) is constant and never dependent on the realm of the air�liquid interface. If the floor rigidity is identical in each alveoli, then the smaller alveolus could have a better pressure and can empty into the bigger alveolus. The first factor is a substance referred to as pulmonary surfactant, which is produced by specialized alveolar cells, and the second is the structural interdependence of the alveoli. Pulmonary surfactant is a posh consisting of about 85�90% lipids and 10�15% proteins. The lipid portion is about 85% phospholipid, roughly 75% of which is dipalmitoyl phosphatidylcholine. Surfactant is also cleared from the alveoli by alveolar macrophages, absorption into the lymphatics, or migration as a lot as the small airways and the mucociliary escalator (discussed in Chapter 31). The medical consequences of an absence of practical pulmonary surfactant occur in a number of situations. Even if their alveoli are inflated for them with positive-pressure air flow, the tendency towards spontaneous collapse is great as a result of their alveoli are much less stable with out pulmonary surfactant. Therefore, the lack of practical pulmonary surfactant in a prematurely born neonate could additionally be a major factor in the toddler respiratory distress syndrome. Pulmonary surfactant can also be essential in maintaining the steadiness of small airways. Alveolar hypoxia or hypoxemia (low oxygen within the arterial blood), or both, could result in a lower in surfactant production or a rise in surfactant destruction. This condition could additionally be a contributing factor within the acute respiratory distress syndrome (also generally known as grownup respiratory distress syndrome or "shock lung syndrome") that may occur in sufferers after trauma or surgery. This process opposes the elevated elastic recoil of the alveoli and the tendency for spontaneous atelectasis to happen due to a scarcity of pulmonary surfactant. Exogenous pulmonary surfactant is now administered immediately into the airway of neonates with toddler respiratory distress syndrome. In summary, pulmonary surfactant helps lower the work of inspiration by reducing the floor pressure of the alveoli, thus decreasing the elastic recoil of the lung and making the lung more compliant. Surfactant also helps stabilize the alveoli by decreasing even additional the surface rigidity of smaller alveoli, equalizing the stress inside alveoli of various sizes. Alveolar Interdependence A second factor tending to stabilize the alveoli is their mechanical interdependence, which was mentioned at the beginning of this chapter. They are mechanically interdependent polygons with flat walls shared by adjacent alveoli. If an alveolus were to begin to break down, it will increase the stresses on the walls of the adjacent alveoli, which might have a tendency to hold it open. This process would oppose a tendency for isolated alveoli with a relative lack of pulmonary surfactant to collapse spontaneously. Conversely, if a complete subdivision of the lung (such as a lobule) has collapsed, as quickly as the primary alveolus is reinflated, it helps to pull different alveoli open by its mechanical interdependence with them. Thus, each pulmonary surfactant and the mechanical interdependence of the alveoli help stabilize the alveoli and oppose alveolar collapse (atelectasis). If the integrity of the lung�chest wall system is disturbed by breaking the seal of the chest wall. Lung volume decreases, and alveoli have a a lot higher tendency to collapse, especially if air strikes in through the wound (causing a pneumothorax) till intrapleural strain equalizes with atmospheric stress and abolishes the transpulmonary pressure gradient. At this point, nothing is tending to carry the alveoli open and their elastic recoil is causing them to collapse. Similarly, the chest wall tends to broaden as a result of its outward recoil is now not opposed by the inward recoil of the lung. When the lung�chest wall system is undamaged and the respiratory muscle tissue are relaxed, the volume of gasoline left in the lungs is decided by the balance of those two forces. Therefore, at excessive lung volumes, the elastic recoil of both the lung and chest wall are inward. The purpose for this lower of about 30% is the effect of gravity on the mechanics of the chest wall, especially the diaphragm. When standing up or sitting, the contents of the stomach are being pulled away from the diaphragm by gravity. When mendacity down, the abdominal contents are pushing inward in opposition to the relaxed diaphragm. This decreases the general outward recoil of the chest wall and reduces the lung volume at which the outward recoil of the chest wall is equal and reverse to the inward recoil of the lungs. These elements are primarily the frictional resistance of the lung and chest wall tissue, and the frictional resistance of the airways to the move of air. Pulmonary tissue resistance is brought on by the friction encountered as the lung tissues transfer in opposition to one another because the lung expands. The airway resistance plus the pulmonary tissue resistance is also known as the pulmonary resistance. Pulmonary tissue resistance usually contributes about 20% of the pulmonary resistance, with airway resistance answerable for the other 80%. Pulmonary tissue resistance may be elevated in such conditions as pulmonary sarcoidosis and fibrosis. Because airway resistance is the major element of the total resistance and since it could enhance tremendously each in healthy people and in these affected by various ailments, the rest of this chapter will concentrate on airway resistance. Turbulent circulate tends to happen if airflow is high, gas density is high, the tube radius is large, or all three situations exist. True laminar circulate probably occurs solely within the smallest airways, the place the linear velocity of airflow is extremely low. Linear velocity (cm/s) is the same as the move (cm3/s) divided by the cross-sectional area.
References
- Makowski GJ, Van Sickels JE. Evaluation of results with threepoint visualization of zygomaticomaxillary complex fractures. Oral Surg Oral Med Oral Pathol 1995;80:624.
- Erickson SJ, Mewissen MW, Foley WD, et al. Stenosis of the internal carotid artery: assessment using color Doppler imaging compared with angiography. AJR Am J Roentgenol 1989;152: 1299-305.
- Na Y, Ye Z, Zhang S: Efficacy and safety of dutasteride in Chinese adults with symptomatic benign prostatic hyperplasia: a randomized, double-blind, parallel-group, placebo-controlled study with an open-label extension, Clin Drug Investig 32(1):29n39, 2012.
- Pritchett JW. Ketorolac prophylaxis against heterotopic ossification after hip replacement. Clin Orthop 1995;314:162- 165.