

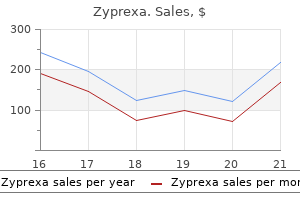
Zyprexa
Christopher D. Chiles, MD
- Assistant Professor of Medicine
- Division of Cardiology
- Texas A&M School of Medicine
- Scott and White Memorial Hospital
- Temple, Texas
Zyprexa dosages: 20 mg, 10 mg, 7.5 mg, 5 mg, 2.5 mg
Zyprexa packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Generic zyprexa 7.5mg with visa
Techniques addressing the lateral crus of the lobular cartilage as a part of tip surgical procedure are reviewed in the part on tip surgery (see web page 272) medicine man trusted 2.5mg zyprexa. In instances where the relationship between the lateral crus and the decrease margin of the triangular cartilage has been misplaced (due to previous surgical procedure in which too much of the cranial margin of the lateral crus has been resected medicine qvar inhaler discount 5 mg zyprexa visa, or on account of trauma) medications on nclex rn buy cheap zyprexa 5 mg, it may be mobilized and shifted (rotated) upward. This process was first described by Rettinger and Masing (1981) using the luxation method. The drawback of the rotation is that it produces torsion between the lateral crus and the dome. Reinforcement the lateral crus is reinforced by a cartilage transplant from septal, auricular, or rib cartilage. Depending on the pathology, reinforcement could additionally be completed by bridging the gap between the cartilages with a thin defend of auricular cartilage. Reconstruction If the lateral crus is severely faulty or atrophic, it may be resected and replaced by a transplant from auricular, septal, or rib cartilage with perichondrium. The graft is medially fastened to the lateral side of the dome (preferably by two sutures) and laterocranial to the caudal margin of the triangular cartilage (by two sutures). This might occur as a outcome of "tip-refining" surgery, when the connections between the higher margin of the lateral crus and the decrease margin of the triangular cartilage have inadvertently been destroyed. It can be seen in aged sufferers because of laxity of the delicate tissues of the lobule. The finish of the lateral crus might then turn into inverted and protrude into the vestibule, resulting in inspiratory breathing obstruction. Resection of the protruding finish of the lateral crus and/or reinforcement of the ala could then be an effective therapy. Reducing Alar Convexity Abnormal convexity or ballooning of the ala is addressed by reducing the spring of the overly convex cartilage. These strategies could weaken the cartilage an excessive amount of, nonetheless, and so they have due to this fact largely been replaced by suture techniques respecting or reconstructing the structural integrity of the alar cartilages. All three methods require a supply approach, both the luxation method or the exterior approach. Gridding Steps A small incision into the vestibular pores and skin overlying the protruding end of the lateral crus is made with No. The lateral protruding part of the lateral crus is dissected subperichondrially using a fragile anatomical forceps and small, barely curved scissors. It should stay sufficiently inflexible to withstand the negative stress in the vestibule during inspiration. Resecting Small Wedges In circumstances with extreme ballooning of the lateral crus, two or three tiny wedges may be resected from the cartilage with a No. These minute resections must be carried out with utmost precision, as this procedure carries a great risk of causing too much loss of alar rigidity. Reducing Alar Concavity In instances where the lateral crus is concave, surgical correction could additionally be indicated for functional (alar collapse on the degree of the vestibule) as properly as aesthetic reasons. In sufferers with a restricted degree of concavity, it may be sufficient to splint it with a batten or strut onlay graft. In other instances, the lateral crus is resected, repositioned by turning it 180 and sutured in a new place. The most secure fixation of the repositioned lateral crus is achieved if each edges overlap. Shortening the Ala by Wedge Resection at Its Base When lowering a distinguished lobule and tip, it could be clever to shorten the ala as part of the process. When the bony and cartilaginous pyramid are lowered, the lobule will turn out to be decrease and wider. To restore the traditional configuration of the lobule, it could then be necessary to bilaterally resect a soft-tissue wedge on the alar base. The lateral crus is exposed and dissected subperichondrially on each side (see page 260). A second incision is made at the higher margin of the wedge that has been outlined. Bipolar coagulation is applied to management bleeding from small branches of the angular artery. Displacing the Alar Base A broad lobular base with a wide floor of the nostril and vestibule may be corrected by medial displacement of the alar base. In the majority of cases, it normally suffices to excise a wedge on the vestibular facet of the vestibular sil. The skin flap is sutured to the lateral a half of the incision at the nasofacial fold. Thinning the Ala In patients with irregular thickness of the lobular skin, it may be advisable to resect a variety of the abundant subcutaneous tissues. Resecting too much soft tissue, or asymmetrical resection leads to ugly retractions which may be virtually irreparable. In this case, the external strategy is advised as it allows the surgeon to work beneath direct view. Narrowing the Lobular Base the lobular base can be narrowed by making one or sometimes two so-called bunching sutures. These narrowing sutures will only be efficient if the gentle tissues have been broadly undermined. The finest results are obtained when the reconstruction is carried out within a few days. It goes past the scope of this book to cope with all kinds of nasal and paranasal pores and skin defects and their surgical correction. Reconstructing the Ala Alar defects are frequent deformities after tumor resection or trauma. It must be barely outsized, as some tissue retraction will take place within the therapeutic course of. It is sutured in place with interrupted pores and skin sutures, each externally and in the vestibule. Inspiratory respiration is commonly impaired in sufferers with a broad, retracted, or indirect columella. Aesthetic complaints could additionally be expressed by sufferers with a slim, short, retracted, hanging, or asymmetrical columella. Protruding Ends of the Medial Crura the decrease ends of the medial crura are abnormally bent in a lateral path. They protrude into the nostril and vestibule the place they might trigger (or contribute to) inspiratory obstruction. Correction is carried out by trimming the protruding ends or approximating the footplates with a suture. A narrow (and long) columella may be a part of a congenitally outstanding, slender pyramid. It may outcome from scarring because of previous surgical procedure (or infection), for instance after transfixion of the membranous septum or surgery of the caudal septal finish. A slim columella may be broadened by an intercrural cartilaginous transplant (columellar strut), or by reconstruction of the caudal septum and a tongue-in-groove method.
Purchase 20mg zyprexa with visa
The plant acquire (lung and thoraco-skeletal system) executes these impulses by various the minute ventilation medications used to treat bipolar buy zyprexa 20mg free shipping. The stage of the loop gain describes the relative change of the system to any breathing disturbance treatment chronic bronchitis discount 5mg zyprexa amex. Periodic breathing at excessive altitude or Cheyne�Stokes respiration are scientific examples of a excessive loop acquire symptoms heart attack women buy zyprexa 10 mg fast delivery. Periodic respiration describes the polysomnographic phenotype of waxing and waning of respiratory circulate and effort, i. The latter is characterised by a chaotic sample of changing breathing frequency and amplitudes of the circulate. Opioids inhibit respiratory rhythms by suppressing brain stem exercise, leading to reduced breathing frequency. Peripheral and central chemosensitivity play a significant function, resulting in a diminished hypoxic and hypercapnic ventilatory response. In essence, opioid-induced sleep apnoea represents a hypercapnic phenotype of sleep apnoea [14]. The substantial variations in prevalence may be because of completely different definitions and affected person populations [18, 19]. These embody excessive titration, post-hyperventilation apnoea, post-arousal apnoea and misclassification of central hypopnoeas [21�24]. Hypoventilation problems Reduction of the minute quantity is a standard attribute of hypoventilation issues. They can generate from all levels of the respiratory system, including insufficient respiratory drive, impaired translation of the respiration impulses from the brain stem by way of the spinal twine and the peripheral nerves to the respiratory muscle tissue, and practical or morphological abnormalities of the thorax and the muscular tissues themselves. Hypoventilation may be a half of difficult respiratory patterns and could additionally be combined with other components as follows. The heterogeneous remedy response may be characterised by variable relative contributions of the loop acquire [29�31], the respiratory drive and the airway obstruction to the evolution of the illness in a person affected person (fig. By contrast, these much less variable, extra managed modes of air flow could also be indicated in patients with airway obstruction, lowered respiratory drive, lowered loop acquire or other hypoventilatory disorders. Thus, a sensible strategy to the sufferers with complicated respiration patterns may be primarily based on the separation of the major pathophysiological elements and on the individual adjustment of the gadget (fig. A description of the (hypothetical) relative contribution of level of the loop acquire and the airway obstruction to the pathophysiology of various phenotypes of sophisticated respiratory patterns. By distinction, hypoventilation problems are characterised by reduced respiratory drive and low loop acquire. The diagram additionally illustrates that the person components could range and this defines their place in the diagram (as symbolised by the closed and dotted circles for opioid-induced sleep apnoea). Whereas, the lower the respiratory drive and the instability the extra ventilatory assist is required. The level of obstruction defines the need for expiratory strain to stabilise the higher and decrease airways. Expiratory stress relief algorithms apply completely different levels during early and end-expiration. The figure reveals the therapeutic choices for addressing the underlying pathophysiological part. The breaths contribute progressively much less as new breaths are continuously added [3]. If a predefined range across the common is exceeded or missed, the algorithms modulate the strain help anti-cyclically. Due to the lowering of the pressure throughout early expiration, the identical tidal volume may be achieved with lower inspiratory pressures. Noninvasive ventilation generates the minute ventilation by a fixed difference between inspiratory and expiratory strain (pressure support, pressure controlled ventilation) or tidal quantity (volume help, quantity controlled ventilation) together with a hard and fast breathing price or back-up frequency. However, these rigid modes may be insufficient or unnecessary for medical conditions with various necessities of the air flow help. Sufficient stress assist during hypoventilation normalises oxygen saturation and prevents a hypoxic ventilatory response. However, the scores have been low at baseline which is a typical finding in Cheyne�Stokes respiration. The patients suffered from quite so much of underlying diseases or comorbidities, including cardiovascular disorders, insomnia and restless legs syndrome, or continual opioid use. The outstanding discount was proven on the second titration evening after randomisation and wishes additional explanation. Moreover, the results are restricted by the high variety of non-evaluable data (30 out of sixty six patients). At baseline, the patients suffered from severe sleep apnoea with overwhelming central disturbances. A recent systematic review recognized five studies involving 127 patients who used opioids for no less than 6 months and were treated with completely different positive stress algorithms. While the gadgets sufficiently eradicated central apnoeas and obstructive occasions, central hypopnoeas nonetheless remained. There was a discrepancy between the variety of manually scored and the saved events in the devices. In conclusion, the algorithms reacted as anticipated in accordance with the scientific experiences. High maximum pressure levels have been experimentally shown to cut back cardiac preload and output in healthy persons. Otherwise, if the patient repeatedly wants higher strain help during the trial it could be advantageous to predefine a further help to stabilise respiration [35]. Treatment failure in some sufferers must be interpreted on the premise of the underlying pathophysiology. The complexity of the breathing disturbances and the comorbidities underlines the relevance of shut supervision and optimal management of the mask interface [35, 44]. Positive airway stress remedy with adaptive servoventilation: half 1: operational algorithms. Respiratory system loop acquire in normal women and men measured with proportional-assist air flow. Periodic inhaling heart failure patients: testing the speculation of instability of the chemoreflex loop. Role of hyperventilation in the pathogenesis of central sleep apneas in patients with congestive coronary heart failure. Risk components for central and obstructive sleep apnea in 450 men and women with congestive coronary heart failure. Central sleep apnea in left ventricular dysfunction: prevalence and implications for arrhythmic danger. The significance and consequence of continuous optimistic airway pressure-related central sleep apnea throughout split-night sleep studies. Central sleep apnea on commencement of continuous optimistic airway stress in patients with a primary analysis of obstructive sleep apnea�hypopnea. Evaluation of a noninvasive algorithm for differentiation of obstructive and central hypopneas. Effects of inhaled carbon dioxide and oxygen on Cheyne-Stokes respiration in patients with heart failure.
Syndromes
- Heavy sweating
- Numbness of mouth and lips
- Vision changes (unusual), including blind spots, blurred vision, changes in how colors look, or seeing spots)
- Help you to be able to do normal activities without asthma symptoms
- Rh incompatibility
- Methadose
- Frequent urination
- Pineapple
Cheap 20mg zyprexa visa
Retrograde (or Inversion) Technique the retrograde (or inversion) method is a relatively atraumatic and safe method to address minor deformities and asymmetries of the lobule and the tip treatment lower back pain buy zyprexa 7.5mg. The sharp angle helps to restore the valve angle in its original position when suturing the incision medications prescribed for depression discount zyprexa 5mg otc. The skin over the lateral crura medicine app order 10mg zyprexa, domes, and interdomal space is undermined in a retrograde direction with totally curved, blunt scissors. The vestibular skin and the perichondrium are dissected from the vestibular aspect of the inverted cartilage. A cranial strip is resected from the inverted lateral crus to refine upwardly rotate the tip. The skin over the lateral crura, domes, and higher part of the medial crura is undermined through the infracartilaginous incision. The lateral crus and dome are pulled out with a hook poked via the cartilage and pores and skin at the inferior margin of the dome. The lateral crus and dome are uncovered with the vestibular skin over a Neivert retractor or the flat, again finish of a chisel. Infracartilaginous Technique In this system, the lateral crura and domes are exposed through an infracartilaginous incision. The infracartilaginous technique provides access to the ala, the lateral crus, and dome, and permits resection, modification, and reinforcement of the cartilage. The incision used on this methodology is way shorter than in the luxation approach and the exterior method. The lateral crus and dome are dissected free utilizing blunt scissors, and delivered by means of a round hook to enable modification beneath direct view. A transcolumellar inverted-V incision and bilateral infracartilaginous incisions are made using a No. The columellar pores and skin is carefully dissected from the caudal margin of the medial crura using pointed, barely curved scissors. Upward dissection of the columellar pores and skin from the medial crura using small, slightly curved scissors or angulated scissors and a fragile, sharp, twopronged retractor. External (or Open) Approach the external (or open) method implies full publicity of the lobular cartilages, cartilaginous vault, bony dorsum, and overlying delicate tissues. It presents superior exposure of the lobular cartilages, the triangular cartilages, the anterior nasal backbone, and the anterior part of the septum. The skin overlying the lobule and the nasal dorsum is elevated via a transcolumellar and two infracartilaginous incisions. The lobular cartilages and the cartilaginous dorsum are uncovered supraperichondrially with pointed, barely curved scissors or angulated scissors. The external approach offers a much wider entry to most nasal constructions than the two aforementioned endonasal approaches. Specific dangers are a drooping tip, and necrosis and scarring of the decrease end of the columellar flap. Nowadays, the external strategy is the method of selection in sufferers with extra extreme deformities and asymmetries of the lobule. It can also be used to reconstruct the anterior septum in sufferers with a cartilaginous saddle nose. This method primarily aims at volume discount of the cranial half of the nasal tip. Too a lot resection could cause weak spot of the lateral nasal wall, and inspiratory collapse. The resections must be carried out symmetrically, especially of the domes, as totally different heights of the remaining cartilages may lead to asymmetric buckling, "bossae," and tip asymmetry. A transcartilaginous incision is made 6 mm cranial to the caudal margin of the lateral crus utilizing a No. Bilateral placement of nice needles from the skin into the vestibule at the level of the planned incisions could help get hold of a symmetrical strategy. A strip of cartilage from the cranial part of the lateral crura (and domes) is then removed, leaving cartilage of sufficient width (minimum 6 mm) behind. Bilateral resection of a cranial triangle of cartilage rotates the nasal tip somewhat upwards. Generally talking, refinement and upward rotation of the nasal tip may be achieved in a extra predictable method by different techniques. Luxation (or Delivery) Technique the luxation or supply approach is a classic way to deal with abnormalities of the lobule, specifically of the tip and alae. The lateral crura, domes, and the upper a half of the medial crura are dissected on each side and delivered outdoors the nostril. The cartilages are exposed on a flat instrument (back finish of a chisel or a Neivert retractor). The lateral crura, domes, and the upper part of the medial crura can now be modified underneath direct view, as required. When wide publicity is required, a columellar strut could additionally be inserted on the finish of the operation to protect support. The skin over the cartilaginous and the decrease half of the bony dorsum is undermined with barely curved, blunt scissors. Cutting these fibers would improve the inspiratory collapsibility of the ala as the dilator muscle contracts throughout inspiration. The connective tissue between the domes and the upper part of the medial crura is slightly loosened. This ought to be done in a conservative method to avoid postoperative drooping of the tip. The ala is lifted with a blunt four-pronged retractor and inverted by stress of the center finger. The cranial margin of the dome is then grabbed with a sharp, round hook utilizing the marks on the skin as points of reference. The incision is started laterally and follows exactly the caudal margin of the cartilage (for details see Chapter four, page 144). A curved hook is poked via the skin and cartilage on the caudal margin of the dome. Care is taken to avoid overstretching or tearing the cartilage and the vestibular pores and skin. They are modified as required by the pathology and the specified modifications (for strategies see web page 272). As publicity is proscribed to the lateral crus, the method provides fewer potentialities but is at the similar time much less traumatic than the luxation method or the external strategy. The caudal margin of the lateral crus is identified and the pores and skin is incised from lateral to medial. When the dome is reached, some further pressure by the middle finger is required to expose the ventricle of the vestibule. The incision is then continued for a couple of millimeters alongside the margin of the medial crus. The lateral crus and dome are now supraperichondrially dissected free from the overlying lobular skin with slightly curved, blunt scissors.
Quality zyprexa 7.5mg
The cartilage or bone will forestall undesired retraction of connective tissue during the healing course of medicine man gallery purchase 10mg zyprexa mastercard. Therefore medications resembling percocet 512 zyprexa 10 mg line, little or no soft-tissue retraction is seen at a caudal septal incision medicine hat generic zyprexa 7.5 mg with visa, whereas unwanted scarring might outcome from a columellar incision, transfixion, vestibular incision, or intercartilaginous incision. Incisions are generally made at right angles to the pores and skin or mucosa for optimal healing. If a disposable blade has been used on rigid tissues, a recent one should be used if further incisions are needed. Incisions should be as brief as possible, but long enough to provide enough entry to the structures and allow the required maneuvers. This applies particularly to incisions used for osteotomies, rasping, and inserting transplants. In surgical procedure of the valve and the cartilaginous dorsum, the intercartilaginous incision may be connected with the caudal septal incision to acquire a sufficiently wide overview. Misnomers From an anatomical or a semantic viewpoint, the names of the next incisions are incorrect. The word transfixion already implies that the tissues are minimize via (Latin: transfigo, -fixi, -fixum = to stab). Hemitransfixion incision: anatomically in addition to linguistically incorrect (see previous text). The variety of stitches applied relies upon not solely on the size of the incision, but also on whether or not the incision was made solely to gain access or additionally to modify sure structures and their relationships. A skinny monofilament synthetic fiber, atraumatically mounted on a round needle, might be the best. It provides entry to the septum, premaxilla and anterior nasal spine, nasal dorsum, columella, and floor of the nasal cavity. Since the surgeon is standing on the best side of the affected person, a right-sided approach means that the devices can be introduced and maneuvered from the proper. The caudal septal end is identified by palpation with the back of the handle of the knife. An incision is made in the pores and skin parallel to the caudal septal margin at a distance of about 2 mm utilizing a No. The incision ought to comply with the full length of the caudal margin of the septal cartilage. Skin, subcutaneous fibers, and perichondrium are gently cut through by a number of delicate strikes of the knife till the cartilage is reached. Care is taken to not minimize into the cartilage, as this will likely cause bending of the caudal finish. Access the caudal septal incision provides entry to the next areas: (1) septum; (2) premaxilla and anterior nasal spine; (3) nasal dorsum; (4) columella; and (5) flooring of the nasal cavity. Septum: Depending on the pathology, the septum is approached by elevating the mucoperichondrium and the mucoperiosteum as mentioned in Chapter 5 (page 159). It is gently closed over the septum after which slowly withdrawn till it slips from the septum. Steps the ala is retracted in a lateral and cranial course with the left hand utilizing an uneven four-pronged hook. The caudal margin of the triangular cartilage is identified with the again of the knife handle. An incision is made from lateral to medial simply above the caudal border of the triangular cartilage using a No. The incision begins midway alongside the lower finish of the cartilage and continues simply past the valve angle. A (bilateral) incision of about 10 mm is long enough to undermine the dorsal pores and skin for repositioning the bony pyramid. A 10-mm incision additionally suffices for inserting crushed cartilage or a small cartilaginous transplant. If the transplant is massive, the method has to be made wider, while the skin has to be undermined over a broader area. For transplants in the supratip and tip area, a really small reduce just above the valve angle may be sufficient. It is used as an method to the paranasal area, the piriform aperture, and the lateral wall of the nasal cavity. If upward rotation of the tip is desired, suturing could also be done in an oblique style by "advancing sutures" this means pulling the tissues above the incision in a medial and cranial course. Steps Access the intercartilaginous incision supplies entry to: (1) the nasal dorsum and the cartilaginous and bony vault; (2) the valve; and (3) the lobule. Only the pores and skin is incised, as chopping through the subcutaneous tissues could trigger abundant bleeding from the angular artery. The incision should be wide sufficient to accommodate the chisels which are to be used for osteotomies. Access the vestibular incision supplies access to: (1) the paranasal space; (2) the piriform aperture; and (3) the lateral wall of the nasal cavity. Lateral wall of the nasal cavity: Access to the lateral wall of the nasal cavity and the inferior turbinate may be gained based on the techniques described in Chapter eight (see web page 311). It is also called the "marginal incision," although this name might give rise to some misunderstanding, as previously discussed. It is used in the external approach in addition to within the luxation approach to ship the lobular cartilages. It may be used as the sole incision for entry to the domes and lateral crura of the lobular cartilage. The Infracartilaginous Incision As Used within the External Approach Steps the infracartilaginous incision is normally produced from medial to lateral. The Infracartilaginous Incision As Used within the Luxation Technique Steps the incision is produced from lateral to medial. The decrease half of the (right) ala is everted with a sharpdull two-pronged hook (dullharp hook for the left ala), while the middle finger of the left hand exerts the mandatory counterpressure. As soon as the primary millimeters of the incision have been made, the hook is repositioned. When the dome is reached, extra stress is exerted by the middle finger to expose the ventricle. The incision is continued by rigorously following the caudal border of the dome and then turning downward over the medial crus. The lateral crus, dome, and the upper part of the medial crus are now supraperichondrially dissected free from the overlying lobular pores and skin with pointed, barely curved scissors. Suturing the infracartilaginous incision is closed with 5 monofilament resorbable sutures. Limited Infracartilaginous Incisions In special instances, a restricted infracartilaginous incision is used, for example when inserting (crushed) cartilage as filler or for reinforcement. This incision may be used as an strategy to the lateral wall of the lobule and the cartilaginous vault.
5 mg zyprexa for sale
Depending on the type of complication medications keppra order 7.5 mg zyprexa visa, a neurosurgeon and/or an ophthalmologist may should medications you cant drink alcohol cheap zyprexa 10 mg otc be consulted symptoms anemia buy zyprexa 20mg lowest price. As to the handling of problems normally and the legal points concerned, we check with Chapter 9, web page 355 and web page 370. Minor Complications essentially the most frequent minor issues of ethmoidal surgical procedure are everlasting crusting, synechiae, closure of the sinus ostia, and neuralgia. Whether or not permanent crusting will outcome is dependent upon the anatomy of the ensuing cavity and the quality of the remaining mucosa. Creating a wider window definitely helps, however this may intrude with restoring nasal and sinus physiology. Leaving a small slip of dressing in the opening for a quantity of days is another choice. Neuralgia could also be associated to the anatomy of the created cavity, a diseased cell, or harm to the anterior or posterior ethmoidal nerve endings. Generally, one should wait no less than 6 to 12 months earlier than deciding to carry out revision surgery, as neuralgic complaints typically subside progressively. Treatment Discussing all of the treatment options for all major issues would go beyond the scope of this book. Although his writings on the means to deal with fresh nasal accidents contain a number of suggestions which might be nonetheless legitimate, he was certainly mistaken on this level. Nasal injuries in childhood, if not correctly handled, might have a fantastic influence on later nasal type and performance. A hematoma that has not been recognized and handled will trigger scarring and retraction of the nasal dorsum, cartilaginous vault, and columella. We have one of the best likelihood to prevent these deformities if we see the patient when the damage remains to be contemporary. Treatment at the moment may stop many of the useful and aesthetic issues that might come up in later life. In describing neonatal nasal deformities, we should always distinguish between nasal deformities due to birth trauma and those occurring in utero. Nasal Deformity as a result of Birth Trauma Nasal deformity within the newborn following vaginal delivery is somewhat widespread. This variation could be very likely due to variations in definition, time lapse between examination and delivery, and ethnic components. The tissues are apparently flattened or pushed throughout start, later returning to their authentic position due to their elasticity. In a minority of instances, nevertheless, the deviation stays and nasal respiratory may be impaired (Jeppesen 1977, 3. Nasal trauma because of vaginal start is characterized by a deviation of the cartilaginous pyramid and lobule to one facet and dislocation of the cartilaginous septum from its base to the opposite aspect. The columella is deviated, while the form of the nostrils and alae is distorted and asymmetrical. Jeppesen and Windfield (1976) postulated that presentation of a kid within the left occipitoanterior position would lead to luxation of the septal base to the proper, whereas presentation in the best occipitoposterior place would trigger luxation to the left. When in addition to the fracture, the ridge of the nostril is depressed or the nostril is laterally dislocated, the recommended plan of action consists of reduction (which should happen within the first few days), the position of wads into the nostrils, and very cautious bandaging. About 30% of all newborns exhibit some flattening of the lobule instantly after birth. This flattening disappears shortly generally, though in some a deformity remains. Although particular person instances of nasal deformity at delivery have been described long ago, the nasal mucosa is decongested and slightly anesthetized by putting a number of drops of xylometazoline 0. Is there loss of assist of the cartilaginous dorsum and tip, indicating a septal dislocation The vestibule, valve, and nasal cavity are inspected using a straight, small diameter endoscope or electric otoscope. When a septal dislocation is found, the cartilaginous septum is gently grasped and examined for irregular mobility utilizing a straight anatomical forceps with protected legs. In babies with respiratory obstruction, isotonic saline or decongestive nose drops are put into the nose before feeding. No youngster reaches puberty without having suffered several minor and major falls and bumps on the nostril. Pathology Septal and pyramid deformities could gradually develop in later life when the septum turns into dislocated from its base by an accident with a frontolateral or basolateral impact. A frontal damage might cause disruption of the cartilaginous pyramid from the bony pyramid. Whether the condition is due to intrauterine trauma or hereditary elements is unclear. This may be acceptable in some circumstances, but in other cases such negligence might have grave consequences. Navigating the gray area between doing too much and too little requires expertise. Plain radiographs have nearly no worth in diagnosing fresh nasal accidents in youngsters. The dad and mom or caregivers should be informed that an correct prediction of the final end result after progress is completed is impossible, and that a second intervention may be indicated after puberty. They pose a major menace, as they often lead to a septal abscess and destruction of the septum. Soft-tissue lesions, corresponding to avulsion of the alae, columella, or the top of the inferior turbinate, should be treated as quickly as possible. This also applies to canine and monkey bites and to lesions of the columella caused by intubation. Wait-and-See Policy When we decide to observe a wait-and-see coverage, the mother and father are requested to be careful for the next developments over the subsequent days: Is nasal respiration attainable, or does the nose stay obstructed Diagnosis the external nostril, septum, and nasal cavity are inspected and palpated after mucosal decongestion beneath common or native anesthesia. A septal hematoma is excluded by palpating the septum with a cotton wool applicator. Closed Correction ("Reduction") In some cases, an immediate correction, or so-called closed discount could additionally be attempted. Steps the nasal mucosa is anesthetized in the ordinary means, and relying on the case, a short general anesthesia could additionally be wanted as properly. With the assistance of a middle speculum and a blunt elevator, the nasal bones are lifted up and repositioned as much as attainable, utilizing three fingers of the opposite hand as an external information. Repositioning of a fresh septal deviation or fractures may also be tried but is usually much less successful. While the bony and cartilaginous pyramid is lifted up by an instrument within the left hand, the septum is repositioned using a blunt or flat instrument in the proper hand. This is necessary to avoid necrosis of the septal cartilage and to stop a septal abscess.
Zyprexa 10 mg overnight delivery
The superior gluteal and pudendal nerves exit the pelvis remote to these three nerves; therefore medicine x xtreme pastillas order 10 mg zyprexa overnight delivery, hip abduction weakness and perineal sensory loss would be essential findings that implicate a sacral plexus damage treatment of tuberculosis discount zyprexa 20 mg overnight delivery. L5 radiculopathy medicine daughter buy 10mg zyprexa free shipping, lumbosacral trunk harm, sciatic nerve injury predominantly involving the frequent peroneal division, and customary peroneal nerve palsy might all have an identical clinical presentation: foot drop. Lumbosacral trunk lesions could also be differentiated from sciatic or frequent peroneal palsies as a end result of they usually trigger weak spot within the posterior tibialis in addition to other extra proximal muscular tissues, together with the gluteals (hip extension and abduction). Differentiating an L5 radiculopathy from a lumbosacral trunk lesion is usually not possible clinically. Imaging (to rule out nerve root compression) and electrodiagnostic testing (to doc paraspinal muscle denervation) assist verify an L5 radiculopathy. A fracture/dislocation of the ipsilateral sacroiliac joint on computed tomographic scan or X-ray might point towards lumbosacral trunk damage in trauma sufferers with a foot drop. Lower sacral plexus (S35) damage causes perineal/perianal sensory loss, decreased anal sphincter tone, loss of an anal reflex, and loss of the bulbocavernosus reflex. Test the bulbocavernosus reflex by briefly flicking the glans penis while your different hand palpates the bulbocavernosus muscle contraction behind the scrotum. Sympathetic fibers destined for the decrease extremity originate from the upper lumbar spinal nerves and enter the sympathetic trunk to be subsequently distributed to the peripheral nerves within the lumbosacral plexus. This section supplies a summary of the respective dermatomes and myotomes for the L1 to S1 spinal nerves. Overall, L2, L3, and L4 radiculopathies ought to be differentiated from femoral neuropathies, L5 radiculopathy from frequent peroneal nerve harm, and S1 radiculopathy from a tibial nerve lesion. The L1 spinal nerve offers sensation to the hypogastric space, groin, and base of the penis/mons pubis. Ilioinguinal, iliohypogastric, and genitofemoral neuropathies, as properly as higher lumbar plexus lesions, are all within the differential prognosis of a suspected L1 radiculopathy. The L2 spinal nerve supplies sensation to the anterior thigh and motor innervation to the iliopsoas muscle. Although each a femoral neuropathy and L2 radiculopathy could trigger anterior thigh pain, numbness, or paresthesias, their motor deficits remain unique: femoral neuropathies cause quadriceps weak spot; L2 radiculopathies cause iliopsoas weakness. The L3 spinal nerve offers sensation to the lower anterior thigh and knee region, along with motor innervation to the quadriceps and hip adductors. Therefore, the principle differential of an L3 radiculopathy can be a femoral neuropathy. Spine imaging and/or electrodiagnostic testing are required to differentiate an L3 radiculopathy from a lumbar plexus lesion. The L4 spinal nerve carries sensation from the medial lower leg, in the saphenous nerve distribution. It offers substantial motor innervation to the quadriceps through the femoral nerve and the hip adductors by way of the obturator nerve. It also provides motor innervation to the anterior tibialis through the widespread peroneal nerve. To differentiate a femoral neuropathy from an L4 radiculopathy one ought to check for hip adductor and foot dorsiflexion weakness, which might be present solely with a radiculopathy. The L5 spinal nerve provides sensation to the anterolateral shin and dorsum of the foot. Therefore, a typical peroneal neuropathy should be dominated out in all L5 radiculopathy sufferers. Fortunately, the L5 nerve root provides motor innervation to different muscular tissues apart from these innervated by the widespread peroneal nerve, including the posterior tibialis and glutei. Therefore, foot inversion (posterior tibialis) should be normal for sufferers with frequent peroneal lesions. The S1 spinal nerve supplies sensation to each the lateral aspect and sole of the foot by way of the sural and plantar nerves, respectively. The S1 nerve root, nonetheless, also innervates the gluteal muscle tissue through the superior and inferior gluteal nerves. Therefore, along with the presence of low back and radicular ache, gluteal weak point helps confirm an S1 radiculopathy. A tibial neuropathy is additional differentiated from both an S1 radiculopathy and a proximal sciatic lesion because it would spare each the gluteal muscle tissue and the extra proximally innervated hamstrings. Structural etiologies embrace tumors, hemorrhage, surgery, obstetric/gynecologic procedures, trauma, and injections. Non-structural etiologies embrace lumbosacral amyotrophic neuralgia, radiation, vasculitis, diabetes, infection, and hereditary pressure palsies. In fact, about one quarter of all pelvic fractures are associated with nerve harm, plexal or otherwise. Most traumatic lumbosacral plexus accidents are postganglionic, secondary to stretch or traction. However, sacroiliac joint fractures or dislocations may very well cause spinal nerve avulsion. As within the cervical area, myelography and magnetic resonance imaging help with the analysis of nerve avulsion by documenting pseudomeningoceles. Considering the proximity of the lumbosacral trunk to the sacroiliac joint, it may be selectively damaged with fracture/dislocations in this space. Because the lumbosacral trunk carries nerves destined for the common peroneal division of the sciatic nerve, these patients current with a foot drop. For classification, traumatic and iatrogenic damage of the lumbosacral plexus may be divided into 4 diagnostic zones, with most sufferers having extra then one zone both utterly or partially involved. Zone 1 entails the anterior divisions of the lumbar plexus (the obturator nerve; medial thigh). Zone 2 209 Lumbosacral Plexus entails the posterior divisions of the lumbar plexus (the femoral and lateral femoral cutaneous nerves; anterior, medial, and lateral thigh/leg). Zone three refers to the anterior divisions of the sacral plexus (the tibial division of the sciatic nerve). Zone four includes the posterior divisions of the sacral plexus (the common peroneal division of the sciatic nerve as nicely as the superior and inferior gluteal nerves). Preliminary knowledge reveal that trauma most regularly includes either the sacral plexus alone or the complete lumbosacral plexus. Patients with regular clotting can also have retroperitoneal bleeds following trauma, retroperitoneal surgery, or groin catheterization. Hemorrhage may be confined to the psoas muscle, iliacus muscle, or belly wall; larger hemorrhages might contain all three. These patients have acute, often severe, again pain radiating to their groin and anterior thigh. Weakness occurs in the quadriceps, iliopsoas, and, sometimes, the hip adductors. There could additionally be sensory loss in a lumbar plexus distribution, principally the groin and anterior thigh.
Water Lily (American White Pond Lily). Zyprexa.
- How does American White Pond Lily work?
- Are there safety concerns?
- Chronic diarrhea, vaginal conditions, diseases of the throat and mouth, and healing burns and boils.
- Dosing considerations for American White Pond Lily.
- What is American White Pond Lily?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96302
Zyprexa 5 mg with amex
It will thus need to medications 2016 discount 5 mg zyprexa visa be mounted in its new place by sutures (and splints) in the reconstruction and fixation section medicine x pop up discount zyprexa 20mg with amex. Double Vertical Chondrotomy Sometimes two vertical chondrotomies behind one another (double vertical chondrotomy) are required for repositioning medicine nelly effective 2.5mg zyprexa. In common, we attempt to chorus from making horizontal cuts within the cartilaginous septum, as they deprive the cartilaginous pyramid of its support. This might result in sagging of the cartilaginous dorsum, until the anterior septum nonetheless rests on the anterior nasal backbone. After disconnecting the cartilaginous septum from the bony septum by a number of vertical chondrotomies, its base will have to be dissected and dislocated from the premaxilla and anterior nasal backbone to create a "swinging door" and provide extensive entry to the posterior septum. Steps Steps the first vertical chondrotomy is made simply anterior to the first fracture line. A second vertical chondrotomy is made both on the second fracture line or at the cartilaginoussseous junction, relying on the deformity. A right-handed surgeon standing on the proper facet of the patient will typically choose to move the cartilaginous plate to the left. The cartilaginous septum has been mobilized and is dislocated to the left with a speculum to obtain extensive access to the bony septum, vomer, and perpendicular plate. However, no cartilage is resected underneath the K area or from the septal base within the area of the anterior nasal spine. Resections in these areas may lead to endorotation of the septal cartilage, which in turn will result in postoperative sagging of the dorsum and retraction of the columella. A cartilaginous and bony crest may impede an try and dissect the septal base from the premaxilla and maxillary crest. Vertical Strips Vertical Strip on the Chondro-Osseous Junction A slender, triangular, vertical strip may be resected at the chondroperpendicular junction to facilitate mobilization of the cartilaginous septum. Horizontal Strips Horizontal Basal Strip A horizontal basal strip could additionally be resected to obtain higher mobility of the septal plate, facilitate its repositioning, and obtain extensive access to the bony septum. Note the two areas the place no cartilage is resected to avoid endorotation of the septal plate. Horizontal Strip at a Horizontal Fracture A horizontal strip will normally should be resected at the degree of a horizontal fracture to enable repositioning of the deviated elements. This too is done in a conservative approach to avoid creating a spot that will result in loss of assist of the dorsum. Bony and Cartilaginous Crest A bony and cartilaginous (basal) crest has normally to be eliminated. A horizontal chondrotomy is made simply above the crest, allowing the cartilaginous a half of the crest to be dissected and removed. If sure components nonetheless tend to deviate, the mucoperichondrium and mucoperiosteum might should be further elevated. A resistant cartilaginous deviation may require an extra vertical or horizontal chondrotomy, or resection of a considerably bigger or additional strip. Sometimes, the cartilaginous septum can solely be straightened by separating it from the triangular cartilages. One ought to by no means depend on "repositioning" the septum utilizing pressure of some kind of endonasal tamponade. Bony and Cartilaginous Deviation A bony and cartilaginous deviation is both resected or fractured into the midline with a strong forceps (Craig type). Resection is carried out via a forceps, bone scissors, or osteotome, relying on the deformity and the thickness of the bone. The resected area is later reconstructed by reimplanting plates of eliminated bone or cartilage. All defective elements of the septal skeleton are repaired by inserting plates of bone or cartilage. Rebuilding the septum serves varied purposes: Maintaining and restoring the support and projection of the cartilaginous pyramid and lobule Restoring the normal stiffness and thickness of the septum, thus preventing well-known sequelae of submucous resection, similar to late perforations, mucosal atrophy, and mucosal fluttering during respiration Facilitating revision surgery Bony Spur A posterior bony spur can only be corrected by resection. A spur is dissected and mobilized using an elevator and an osteotome, and eliminated with a forceps. Inserting small plates of bone and cartilage, made by cutting or barely crushing resected components, due to this fact suffices. It is a precondition of an excellent practical and aesthetic result, and it could prevent complications similar to postoperative bleeding, hematomas, ecchymosis, and edema. Various strategies may be used, corresponding to inner dressings, special sutures, or internal and exterior splinting. The alternative relies upon upon the kind of surgical procedure carried out and the non-public desire of the surgeon. A lengthy speculum is placed into the septal house, and remnants of blood are eliminated by suction to avoid a septal hematoma. Small plates of bone (or cartilage, if inadequate bone is available) are inserted into the posterior septal house utilizing a long bayonet forceps. These small plates are created from the resected bony and cartilaginous septum, either by cutting or using a crusher. The pieces of bone and/or cartilage are positioned mosaicfashion on the inside of the left mucosal flap. The mucosal flaps are introduced together by adjusting the interior dressings intranasally. Internal Dressings Internal dressings are used to hold the reconstructed septum in the midline and prevent a septal hematoma. They may also serve to support the nasal bones and cartilaginous pyramid in their new place. These dressings encompass a polyvinyl acetate sponge impregnated with oxidized cellulose. The septal house is closed by bringing the 2 mucosal flaps gently along with the internal dressings, using the blunt finish of the elevator. A posterior septal defect is repaired by inserting plates of bone or cartilage with an extended (14 cm) bayonet forceps (see Phase 5: Reconstruction). Many surgeons apply the interior dressings on the very end of the operation, after closing all incisions. Others favor to apply the self-expanding internal dressings first, close the septal house, reconstruct the posterior septum, and then lastly fixate the anterior septum in place and suture the various incisions. The internal dressing is mounted to the nasal dorsum to prevent it from slipping into the nasopharynx. Sutures and Splints Guide Sutures Guide sutures are used to maneuver the cartilaginous and bony plates into position. Just before closing, a small reduce is made into the frenulum to bury the suture deep to the mucosa. Septospinal Suture If the septal base has the tendency to slip off the anterior nasal spine and premaxilla, the septal plate may be held in place by a septospinal suture. A slowly resorbable three suture is handed through the septal base, downward by way of the connective tissue fibers and the buccal mucosa on the left side of the anterior nasal backbone and the frenulum of the upper lip, after which again through the mucosa and the connective tissue on the proper aspect of the nasal spine.
Discount zyprexa 7.5 mg fast delivery
Composition of body fluid As well as water xanax medications for anxiety buy discount zyprexa 10 mg online, physique fluid consists of dissolved substances medicine names generic zyprexa 10mg fast delivery, corresponding to electrolytes (sodium medications ordered po are cheap 10 mg zyprexa with mastercard, potassium and chloride), gases (oxygen and carbon dioxide), vitamins, enzymes and hormones (Nair, 2011). In addition, waste products, corresponding to urea, phosphates, minerals, ketones from the metabolism of fats and nitrogenous waste from the breakdown of protein, are transported out of the physique via the kidneys as urine. If physique temperature rises above the consolation zone of round 37, the blood vessels close to the surface of the the cell Chapter 4 pores and skin dilate, releasing a few of the warmth. In addition, sweat glands release sweat (which is 99% water) when the physique temperature rises. Provides lubrication for the linings of organs and passages in the physique; for instance, swallowing is made simpler by the oesophagus being lubricated. Is a part of saliva, providing lubricant to meals, and aiding chewing, swallowing and digestion. Has a protecting functionwashes away particles that get within the eyes as well as offers cushioning against shock to the eyes and the spinal wire. Is a component of amniotic fluid, which offers protection for the fetus during being pregnant. Some of the problems related to water deficiency embody:low blood stress blood clotting renal failure severe constipation multisystem failure greater risk of infection electrolyte imbalance. The composition of electrolytes differs between the intracellular and extracellular compartments, and fluid steadiness is linked to electrolyte stability. Electrolytes affect:the amount of water in the physique the acidity of blood (pH) muscle operate different essential processes. The body loses electrolytes by way of sweating or not taking in enough fluids to preserve their presence in acceptable numbers. Helps to keep normal nerve and muscle perform; maintains common coronary heart fee, regulates blood glucose and blood pressure. Essential for the digestion of proteins, carbohydrates and fat and absorption of calcium. Function of electrolytes Electrolytes are particularly important for the physique because they: 1. Help to keep the acidase balance, which is critical for normal mobile activity. In order for the physique to operate properly, it should be capable of preserve electrolyte levels within very slim limits. Controlled by signals from hormones, these electrolyte ranges are maintained by the movement of electrolytes into, and out of, cells, as required. If the balance of electrolytes is disturbed, and an imbalance occurs, many critical disorders can develop. This can occur if somebody: 83becomes dehydrated from issues similar to diarrhoea, vomiting, profuse sweating, poor diet and poor consumption of fluids; turns into over-hydrated (water toxicity) by way of consuming too much water or infusing inappropriate quantities of intravenous fluids; takes certain drugs, such as laxatives and/or diuretics; has certain medical issues, corresponding to coronary heart, liver and kidney issues. Severe dehydration may end up in circulatory issues, including tachycardia (rapid heartbeat), as well as problems with the nervous system, resulting in a loss of consciousness or shock (Nair, 2011). With the high proportional fluid body weight of neonates and infants, and the fact that infants and kids are extra susceptible to catching infectious ailments, usually accompanied by diarrhoea and vomiting, it becomes apparent that infants and youngsters are at a excessive threat of developing electrolyte imbalanceseither briefly or permanently. Aldosterone is a steroid hormone produced by the adrenal glands and regulates electrolyte and fluid steadiness by growing the reabsorption of sodium and water and the release of potassium within the kidneys, which in flip increases blood volume and blood pressure. This is a hormone secreted by heart muscle cells (myocytes) and is a strong vasodilator. It is involved within the homeostatic control of body water, sodium, potassium and fat (adipose tissue). It is released by myocytes within the atria of the guts in response to high blood pressure and it reduces the water, sodium and adipose loads on the circulatory system, thereby lowering blood stress. Atrial natriuretic peptide Conclusion this ends this chapter on the topic of cells. Cells are extraordinarily complicated parts of the body, however an understanding of them and their capabilities is important in allowing us to understand how the human body itself capabilities. Chapter 4 the cell Activities eighty four Now evaluation your learning by finishing the training activities on this chapter. The net passive movement of molecules or ions due to their kinetic power from an space of upper to certainly one of lower concentraDown 1. A semipermeable organic structure separating the interior of the cell from the surface surroundings 9. In order for the to perform correctly, it must have the power to keep levels within very limits. Controlled by indicators from, these levels are maintained by the movement of electrolytes into, and out of, cells, as required. The cell Choose from: energetic physique cell electrolyte passive alerts wide electrolyte hormones mitochondrial slender Chapter four osmotic 2. Although is the commonest type of protein-mediated transport throughout the cell, it tends to be overshadowed by. Choose from: active transport diphosphate facilitated diffusion power protoplasm membrane routes solutes solvents pumped gradient adenosine gradients eighty five Wordsearch 1. Aggregate: a set of things that are gathered collectively to kind a total quantity. Cellular matrix: an insoluble, dynamic gel within the cytoplasm, which is believed to be concerned in cell form willpower and movement. Equilibrium: a situation by which all appearing influences are cancelled by each other, so resulting in a secure and balanced condition. Eukaryotic cells: these are cells that usually embody, or have included, chromosomal materials inside one or more nuclei. The cell Haemolysis: Homeostasis: the rupturing of red blood cells (erythrocytes). Hormone: a chemical released by one or more cells that affects cells in different components of the organismessentially a chemical messenger that transports a signal from one cell to another. Metabolism: this word describes all chemical reactions involved in sustaining the dwelling state of the cells and the organism, and may be conveniently divided into two categories, particularly catabolism (the breaking down of molecules to be able to obtain energy) and anabolism (which is the synthesis of compounds that the cells have to survive and perform). Neurotransmitter: a chemical that allows the transmission of indicators from one neurone to the following throughout a synapse. Osmotic pressure: the stress required to prevent the movement of pure water (containing no solutes) into an answer containing some solutes when the options are separated by a selective permeable membrane. Passive transport: the process by which substances move on their very own down a concentration gradient with out using mobile power. Selective permeable membrane: a membrane that allows the unrestricted passage of water, but not solute molecules or ions. Solubility: the property of a chemical substance (the solute) to dissolve in a solvent so as to kind a homogeneous solution of the solute. Synthesis: this word within the context of this subject usually means creation/production/ manufacture. Enclosed by lipid bilayer, vesicles can type naturally; for instance, during endocytosis (protein absorption). Vickers Aim To introduce the student to the fascinating and essential topic of genetics, in order that a data of genetics will permit them to understand lots of the illnesses which have a genetic underpinning. Learning outcomes On completion of this chapter the reader will be capable of:Understand genes and their importance to our health status.
Cheap zyprexa 2.5mg without a prescription
Paraspinal denervation is also indicative of preganglionic or intraforaminal nerve harm medications enlarged prostate order 10mg zyprexa with mastercard. My examination routine is divided into six distinct steps (See Box: Six steps of a complete brachial plexus examination (p treatment uveitis zyprexa 7.5mg mastercard. Six steps of a comprehensive brachial plexus examination Back Observation Rhomboids Latissimus dorsi Trapezius Scapular winging Shoulder Supraspinatus Deltoid Posterior deltoid Teres main Pectoralis major Infraspinatus Arm Triceps Biceps Brachioradialis Forearm Supinator Pronator Wrist flexion Wrist extension Finger extension Hand Observation Finger flexion 132 Clinical Evaluation of the Brachial Plexus Thenar intrinsics Hypothenar intrinsics Interossei Lumbricals Skin Sensation Perspiration/Horner syndrome Pulses/masses Reflexes/Tinel sign Step 1: Back medications in carry on luggage quality zyprexa 5mg. The presence at rest of scapular winging, muscle atrophy, and asymmetry of the shoulders and scapulae are noted. Next, the affected person shrugs the shoulders upward to allow evaluation of trapezial and levator scapulae function. Having the affected person deliver the scapulae collectively allows assessment of the rhomboids. The latissimus dorsi are palpated bilaterally, and the patient is requested to cough, which causes their contraction. The affected person is instructed to raise the arms to the facet and straight above the head to verify trapezial operate. Next, the patient is told to attain toward the wall with the affected arm, and scapular winging is evaluated. Starting with the arm straight and to the facet, the patient is instructed to abduct the arm. With the arm horizontal to the floor, the posterior head of the deltoid (posterior movement) and teres main (downward movement) are examined. The patient then flexes the forearm 90 levels ("hold-up" position), and each the clavicular (lateral pectoral nerve) and sternal (medial pectoral nerve) heads of the pectoralis main are assessed, both visually and by palpation. The triceps are examined with the upper arm parallel to the floor, so the effect of gravity is eradicated. Elbow flexion is examined with the forearm each totally supinated (biceps brachii) and half supinated (brachioradialis). The affected person flexes the wrist (flexor carpi radialis and ulnaris), after which the arm is pronated and the wrist extensors are tested (extensor carpi radialis longus and brevis and extensor carpi ulnaris). With the forearm positioned on a flat surface, the long forearm finger extensors (extensor digitorum communis, extensor indicis, extensor digiti minimi, and extensor pollicis longus and brevis) are evaluated. The affected person is then instructed to open and shut the hand so that any evidence of contracture can be observed, if present. Next, the thumb is evaluated further, together with abduction, adduction, opposition, and flexion. Flexion on the proximal (flexor digitorum superficialis) and distal (flexor digitorum profundus) interphalangeal joints is assessed. Abduction and opposition of the fifth digit are evaluated, in addition to any Wartenberg or palmaris brevis indicators. Finger abduction (dorsal interossei), adduction (palmar interossei), and extension on the interphalangeal joints are tested (lumbricals). Fingertip testing is especially important, contemplating that the thumb, lengthy finger, and fifth digit represent completely different dermatomes. Any abnormality or asymmetry between the higher extremities is evaluated further, together with evaluation of two-point discrimination and localization. This emergent analysis, nonetheless, is often limited by different accidents, together with long-bone fractures, backbone trauma, and affected person confusion or stupor. This screening examination, or main survey, evaluates 9 muscle tissue which were selected because they each comply with a separate path via the brachial plexus (Table 5. Finally, hand movements are tested, including the flexor carpi radialis, extensor indicis, abductor pollicis brevis, and dorsal interossei. If the first survey reveals a deficit, a secondary survey within the emergency division contains sensory and additional motor testing. Proximal lesions are then examined using a spinal nerve template (which spinal nerves are affected To perform the secondary survey, think of all the muscular tissues innervated by the injured factor (as determined by the first survey. A comprehensive examination (described previously) should always be carried out; however, in plenty of trauma sufferers, that is completed later when the affected person is totally cooperative and more time is out there. Other, less frequent etiologies embody compression by anomalous fibrous ridges on the scalene musculature (neurogenic thoracic outlet syndrome), one hundred thirty five Clinical Evaluation of the Brachial Plexus delayed radiation damage, and acute brachial plexitis (Parsonage-Turner syndrome). The supply of irritation for neurogenic thoracic outlet syndrome is localized to the scalene triangle. The scalene triangle is made up of the anterior scalene anteriorly, the middle scalene posteriorly, and the edge of the first rib inferiorly. Irritation of the brachial plexus is often from an irregular fibrous band, on or near these two scalene muscles. An elongated C7 transverse course of or cervical rib could also be present, each of which unfavorably reorient the scalene muscles, probably resulting in neural compression or irritation. The affected person with traditional neurogenic thoracic outlet syndrome has forward-drooping shoulders. Manifestations of neurogenic thoracic outlet syndrome are often localized to the C8 and T1 spinal nerves. Sensory loss, when current, happens on the medial aspect of the forearm, in addition to on the medial third of the hand. Hand intrinsic weak point and atrophy are often extra median than ulnar, whereas sensory loss is all ulnar (ulnar and medial antebrachial cutaneous nerves, both from the medial cord). Externally rotating the arm whereas abducting it above the top often precipitates or worsens symptoms after a minute or two on this position (Roos maneuver or elevated arm stress test). An apical lordotic cervical radiograph documents a cervical rib or elongated C7 transverse course of, when present. Care have to be taken to differentiate thoracic outlet syndrome from C8 radiculopathy or ulnar compression on the elbow. Concurrent weak point in median (abductor pollicis brevis) as well as ulnar (abductor digiti minimi or the primary dorsal interosseous) innervated muscles helps verify a extra proximal harm to the brachial plexus. No historical past of neck or radicular ache, together with the presence of each C8 and T1 sensory and motor adjustments, helps exclude a single-level radiculopathy. The commonest damage is an Erb palsy, where C5 and C6 (or the upper trunk) are broken. Another type of start damage is Klumpke palsy, with damage to the C8 and T1 nerve roots. Although this palsy can happen during a breech supply, with the arm hyperabducted above the pinnacle, it mostly occurs after a face-first supply where the top is hyperextended. Other forms of delivery brachial plexus damage embrace complete plexal harm and an Erb plus palsy. The prognosis of both Klumpke palsy and complete brachial plexus palsy are considerably worse than that for Erb palsy. Neurological prognosis of an obstetrical palsy relies greatly on observing the arm and hand position at rest, a lack of movement, and higher extremity asymmetry throughout play and crawling. Electrodiagnosis ought to be first performed four to 6 weeks after harm, after which on a serial foundation (approximately each three months) to assess recovery.
Order 5mg zyprexa visa
The deltoid is the prime abductor of the arm treatment zinc toxicity buy zyprexa 7.5mg with mastercard, especially between 30 and ninety levels symptoms after conception cheap zyprexa 10mg amex. The preliminary 30 levels of abduction is primarily managed by the supraspinatus symptoms rotator cuff tear discount 2.5mg zyprexa otc, whereas abduction above ninety degrees has an necessary trapezial element, a muscle that rotates the shoulder girdle upward. Abducting the arm to the facet and slightly in entrance of the body checks the anterior and lateral heads of the deltoid. The absence of posterior deltoid contraction might help affirm an axillary palsy, particularly in those patients with a strong supraspinatus muscle that alone can abduct the arm to ninety levels. Arm flexion at the shoulder (in entrance of the body) is mediated by the anterior deltoid. The axillary nerve passes via the quadrangular space, which is bordered superiorly by the teres minor, inferiorly by the teres main, laterally by the neck of the humerus, and medially by the long head of the triceps. The axillary nerve is often injured in isolation by shoulder trauma, together with shoulder dislocations or humeral fractures. Immediately after passing through the quadrangular house, the axillary nerve divides into anterior and posterior divisions. The anterior division curves anterior and somewhat superior beneath the deltoid muscle, which it innervates. The posterior division provides a direct branch to the teres minor after passing via the quadrangular area, after which becomes subcutaneous by piercing the brachial fascia. By examining the latissimus dorsi (the thoracodorsal nerve), as nicely as all of the muscle tissue innervated by the radial nerve, posterior twine involvement could be excluded. The axillary nerve may be compressed on the quadrangular house, which is named the quadrangular house syndrome. Even with full deltoid paralysis, sufferers may use other upper-extremity muscular tissues to abduct the arm, thereby mimicking deltoid function. This cutaneous extension of the axillary nerve carries sensation from the higher lateral arm and is called the upper lateral brachial cutaneous nerve. In addition, both the coracobrachialis and the long head of the triceps, which connect the scapula to the humerus and olecranon, respectively, can substitute for deltoid perform by lifting the arm. Abducting the arm to the facet, and slightly in entrance of the body, checks the anterior and lateral heads of the deltoid. Aside from the main terminal branches, every twine has different smaller, "minor" branches: the lateral twine has one; each the medial and posterior cords have three. The lateral pectoral nerve concentrates its innervation upon the clavicular head of the pectoralis major. Then, towards resistance on the medial elbow, have the affected person swing the arm toward midline. Then, against resistance at the medial elbow, instruct the affected person to swing the arm anterior toward midline (across the chest). The medial pectoral nerve (C61) innervates the pectoralis minor, which it passes by way of, after which pierces the clavipectoral fascia to innervate the sternal head of the pectoralis main. As mentioned, this nerve nearly always communicates with the lateral pectoral nerve. To test the sternal head of the pectoralis major, the affected person ought to begin with the elbow flexed ninety levels and the arm kidnapped approximately 30 levels. Then instruct the patient to adduct the arm against resistance utilized to the medial elbow. Just previous to formation of the ulnar nerve, the medial wire gives off two branches: the medial brachial cutaneous nerve and the medial antebrachial cutaneous nerve. In summary, sensory loss on the medial one half of the upper arm (medial brachial cutaneous) and forearm (medial antebrachial cutaneous) must be used to confirm involvement of the medial twine. Therefore, the medial brachial cutaneous nerve returns sensation by way of the medial wire and lower trunk to the T2 spinal nerve. The presence of T2 axons within the brachial plexus has been excluded thus far for simplicity. Instruct the patient to adduct the arm against resistance when you examine the teres main. All three of those branches hang down like icicles from the posterior wire over the floor of the subscapularis muscle. The first and last of those minor branches from the posterior cord are aptly named the higher and decrease subscapular nerves (C5, C6). The subscapularis muscle (along with the teres major, latissimus dorsi, and pectoralis major) internally rotates the arm. The decrease subscapular nerve innervates the lower half of the subscapularis muscle, in addition to the teres main. The teres main, along with the latissimus dorsi and pectoralis major, are the main arm adductors. To take a look at the teres main, begin with a straightened arm abducted horizontally with the palm down. The different minor department from the posterior twine is the thoracodorsal nerve, which arises between the upper and decrease subscapular nerves. In abstract, the entire branches from the posterior cord act to adduct and internally rotate the arm. The onerous part is over; connecting the proximal and distal ends of the plexus is straightforward. The anterior divisions from the upper and middle trunks create the lateral cord; solely the anterior division of the decrease trunk forms the medial twine. The posterior cord receives the largest variety of divisions (three); this could be remembered by the truth that the posterior twine subsequently yields the biggest terminal department of the plexus, the radial nerve. In this case, a extra distal, accessory communication from the lateral twine to the ulnar nerve is normally current, which carries this C7 enter. It is intimately related to numerous muscular, arterial, and venous buildings because it passes through these regions. The proximal brachial plexus is positioned throughout the posterior triangle of the neck. This posterior triangle is outlined by the sternocleidomastoid muscle anteriorly, the trapezius posteriorly, and the clavicle inferiorly. The posterior belly of the omohyoid traverses the lower facet of the posterior triangle, converging with the suprascapular nerve on the scapula. The brachial plexus passes by way of the interscalene triangle, which is outlined by the anterior scalene, center scalene, and first rib. The apex of 111 Brachial Plexus Anatomy the interscalene triangle is located in the posterior triangle of the neck. The anterior and center scalenes originate from the anterior and posterior tubercles, respectively, of multiple cervical transverse processes. These muscles run down and connect along the primary rib, with the spinal nerves and brachial plexus being sandwiched between them. The region where the brachial plexus and subclavian artery exit from between the scalenes and over the primary rib is a potential web site of entrapment (thoracic outlet syndrome). The brachial plexus divisions lie deep to the clavicle, whereas the cords and their branches are deep to the pectoralis minor and coracoid process. In the axilla, the brachial plexus cords lie between the clavipectoral fascia (superficial) and subscapularis muscle (deep).
References
- Hemal AK, Mukherjee S, Singh K: Laparoscopic pyeloplasty versus robotic pyeloplasty for ureteropelvic junction obstruction: a series of 60 cases performed by a single surgeon, Can J Urol 17(1):5012n5016, 2010.
- Plow EF, Felez J, Miles LA. Cellular regulation of fibrinolysis. Thromb Haemost 1991;66:132-6.
- Petersen JL, Mahaffey KW, Hasselblad V, et al. Efficacy and bleeding complications among patients randomized to enoxaparin or unfractionated heparin for antithrombin therapy in non-ST-Segment elevation acute coronary syndromes: a systematic overview. JAMA 2004;292:89-96.
- Aucouturier P, Barra A, Intrator L, et al. Long lasting IgG subclass and antibacterial polysaccharide antibody deficiency after allogeneic bone marrow transplantation. Blood. 1987;70:779-785.
- Goto Y, Koga S, Horai S, Nonaka I. Chronic progressive external ophthalmoplegia: a correlative study of mitochondrial DNA deletions and their phenotypic expression in muscle biopsies. J Neurol Sci. 1990;100:63-69.