

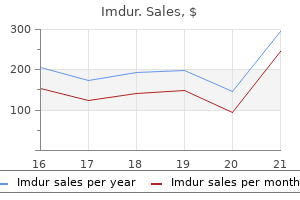
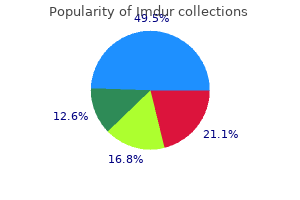
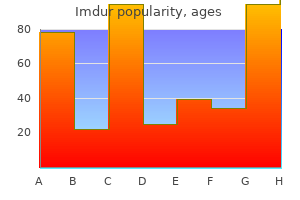
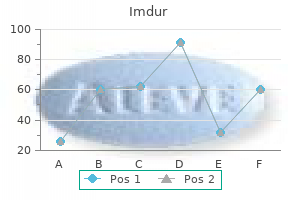
Imdur
Amanda L. O’Donnell BDS, MFDS (Eng), MClin Dent, MPaedDent, FDS RCS (Eng)
- Consultant in Paediatric Dentistry,
- UCL Eastman Dental Institute, London, UK
Imdur dosages: 40 mg
Imdur packs: 30 pills, 60 pills, 90 pills, 120 pills, 240 pills, 180 pills, 360 pills

Purchase 20mg imdur with amex
The clinical manifestations and morphology of those two species are very related and are therefore mentioned together pain medication for dog hip dysplasia buy discount imdur 40 mg line. Etiology and Pathogenesis Humans are the only definitive host for the grownup stage of T spine diagnostic pain treatment center purchase imdur 40mg line. The tapeworms fibroid pain treatment relief cheap 20 mg imdur visa, which can reach 8 m in length with 1000�2000 proglottids, inhabit the higher jejunum. The embryo released after ingestion invades the intestinal wall and is carried to striated muscle or viscera, the place it transforms into the cysticercus. After the cysticercus is ingested, it takes ~2 months for the mature adult worm to develop. The proglottids are often motile, and patients may experience perianal discomfort when proglottids are discharged. Mild stomach ache or discomfort, nausea, change in appetite, weakness, and weight reduction can happen. Prevention the main technique of stopping infection is the enough cooking of beef or pork viscera; publicity to temperatures as low as 56�C for 5 min will destroy cysticerci. Refrigeration or salting for lengthy intervals or freezing at -10�C for 9 days also kills cysticerci in beef. The tapeworm, often ~3 m in length, could have as many as one thousand proglottids, every of which produces as a lot as 50,000 eggs. Proglottids are released and excreted into the feces, and the eggs in these proglottids are infective for each people and animals. Autoinfection may happen if an individual with an egg-producing tapeworm ingests eggs derived from his or her own feces. The medical presentation of cysticercosis is determined by the quantity and site of cysticerci in addition to on the extent of related inflammatory responses or scarring. Seizures are associated with inflammation surrounding cysticerci within the mind parenchyma. An immunoblot assay using lentil lectin purified glycoproteins is >99% particular and highly sensitive. However, patients with single intracranial lesions or with calcifications could additionally be seronegative. All of the diagnostic antigens have been cloned, and assays using recombinant antigens are being developed. These assays are solely classified on the premise of the location and viability of the parasites. Left: Magnetic resonance imaging showStudies have demonstrated that cliniing a cysticercus in the lateral ventricle, with resultant hydrocephalus. The arrow points to the cal criteria can help in diagnosis in chosen scolex throughout the cystic parasite. In sufferers from endemic areas who ment of the cyst wall and an inner scolex (arrow). Right: Multiple cysticerci, including calcified had single enhancing lesions presenting lesions from prior an infection (arrowheads), viable cysticerci in the basilar cisterns (white arrow), with seizures, a normal bodily examinaand a large degenerating cysticercus in the Sylvian fissure (black arrow). Finally, spontaneous decision or hydrocephalus could develop papilledema or display altered psychological decision after therapy with albendazole alone is in maintaining with status. When cysticerci develop at the base of the brain or within the sub- neurocysticercosis. Minor diagnostic standards embody neuroimaging findings consistent arachnoid area, they may cause persistent meningitis or arachnoiditis, with however less attribute of cysticercosis, medical manifestations sugcommunicating hydrocephalus, hemorrhages, or strokes. Demonstration of cysticerci by histologic or microscopic examination certainty is feasible only with particular demonstration of the parasite of biopsy materials (absolute criteria). Visualization of the parasite within the eye by funduscopy vation of the parasite in excised tissue, by funduscopic visualization of c. Neuroradiologic demonstration of cystic lesions containing a characterthe parasite within the eye (in the anterior chamber, vitreous, or subretinal istic scolex spaces), or by neuroimaging studies demonstrating cystic lesions con2. Neuroradiologic lesions suggestive of neurocysticercosis of neuroimaging studies, the scolex can now be identified in many b. In other situations, a clinical diagnosis is predicated on a combinaimmunoelectrotransfer blot tion of medical presentation, radiographic studies, serologic exams, and c. Resolution of intracranial cystic lesions spontaneously or after remedy exposure historical past. Lesions compatible with neurocysticercosis detected by neuroimaging embody cystic lesions with or with out enhancement. Clinical manifestations suggestive of neurocysticercosis ated enhancement), or focal enhancing lesions. Demonstration of antibodies to cysticerci or cysticercal antigen in cerebrospinal fluid by enzyme-linked immunosorbent assay lesions in the subarachnoid space or fissures might enlarge up to 6 cm in diameter and may be lobulated. The diagnosis is confirmed in sufferers with both one absolute criterion or a mix of two main criteria, one minor criterion, and one epidemiologic criterion (Table 260-1). Recent knowledge suggest that both medical or surgical remedy can be used for spinal illness. The prevention of cysticercosis includes minimizing the alternatives for ingestion of fecally derived eggs by the use of good private hygiene, effective fecal disposal, and treatment and prevention of human intestinal infections. Mass chemotherapy has been administered to human and porcine populations in efforts at disease eradication. Finally, vaccines to prevent porcine cysticercosis have proven promise in studies and are under growth. These infections are prevalent in most areas the place livestock is raised in association with dogs. These parasites are discovered on all continents, with areas of excessive prevalence in China, central Asia, the Middle East, the Mediterranean area, eastern Africa, and elements of South America. After the ingestion of eggs, cysts develop within the intermediate hosts-sheep, cattle, people, goats, camels, and horses for the E. The gravid phase splits to launch eggs which are morphologically much like Taenia eggs and are extremely hardy. Daughter cysts develop from the inner side of the germinal layer, as do germinating cystic constructions called brood capsules. Because a period of years elapses earlier than cysts enlarge sufficiently to cause signs, they might be discovered by the way on a routine x-ray or ultrasound research. The preliminary administration of neurocysticercosis ought to focus on symptom-based treatment of seizures or hydrocephalus. If parenchymal lesions resolve without development of calcifications and patients remain free of seizures, antiepileptic remedy can often be discontinued after 1�2 years. Placebo-controlled trials are clarifying the medical benefit of antiparasitic medication for parenchymal neurocysticercosis. For the treatment of sufferers with mind parenchymal cysticerci, most authorities favor antiparasitic medicine, together with albendazole (15 mg/kg per day for 8�28 days) or praziquantel (50�100 mg/kg daily in three divided doses for 15�30 days). A combination of albendazole and praziquantel (50 mg/kg per day) may be more effective in patients with multiple lesions.
Purchase imdur 20 mg on line
Although primary prevention is difficult neuropathic pain treatment guidelines iasp order 20 mg imdur fast delivery, the degree of residual left ventricular dysfunction despite optimum medical therapy (35%) to enable for adequate transforming and the underlying etiology (post�myocardial infarction or ischemic cardiomyopathy) are the two single most necessary risk markers for stratification of need and profit pain treatment wellness center generic imdur 40 mg without a prescription. Revascularization is most robustly supported in people with ongoing angina and left ventricular failure ankle pain treatment running discount imdur 20 mg with mastercard. Revascularizing those with left ventricular failure in the absence of angina remains controversial. There was no vital difference between teams with respect to the primary endpoint of death from any cause. Cardiac signs and train tolerance improved from baseline to a similar degree in both research teams. However, left ventricular aneurysm surgery remains to be advocated in these with refractory coronary heart failure, ventricular arrhythmias, or thromboembolism arising from an akinetic aneurysmal phase of the ventricle. Investigations that use both bone marrow�derived precursor cells or autologous cardiac-derived cells have gained traction. [newline]A number of small- and moderate-scale trials of such therapy have centered on post�myocardial infarction patients and have used autologous bone marrow�derived progenitor or stem cells. These trials have had variable results, with most demonstrating modest improvements in parameters of cardiac structure and remodeling. Two preliminary pilot trials delivering cells by way of an intracoronary approach have been reported. In another, cardiosphere-derived cells grown from endomyocardial biopsy specimens have been used. These small trials demonstrated improvements in left ventricular perform but require far more work to usher in a clinical therapeutic success. The applicable route of administration, the quantity of cells to obtain a minimal therapeutic threshold, the constitution of these cells (single supply or mixed), the mechanism by which benefit accrues, and short- and long-term security remain to be elucidated. Several methods of gene supply have been developed, including direct intramyocardial injection, coronary artery or venous infusion, and injection into the pericardial house. Cellular targets into account include 2-adrenergic receptors and calcium biking proteins similar to inhibitors of phospholamban. Stromal-derived factor 1 enhances myocardial repair and facilitates "homing" of stem cells to the location of tissue injury. Strategies utilizing intramyocardial injections to deploy this gene at sites of injury are being studied. More advanced therapies for late-stage heart failure similar to left ventricular help devices and cardiac transplantation are lined intimately in Chap. Recurrent coronary heart failure and associated cardiovascular conditions account for only half of readmissions in sufferers with heart failure, whereas other comorbidity-related situations account for the remaining. The key to achieving enhanced outcomes should begin with the eye to transitional care on the index hospitalization with facilitated discharge by way of complete discharge planning, affected person and caregiver training, appropriate use of visiting nurses, and planned follow-up. Early postdischarge follow-up, whether or not by phone or clinic-based, may be crucial to ensuring stability as a outcome of most heart failure�related readmissions are inclined to happen inside the first 2 weeks after discharge. Although routinely advocated, intensive surveillance of weight and important signs with use of telemonitoring has not decreased hospitalizations. Intrathoracic impedance measurements have been advocated for the identification of early rise in filling strain and worsened hemodynamics so that preemptive management may be employed. Once coronary heart failure becomes advanced, regularly scheduled evaluation of the disease course and options with the patient and family is beneficial together with discussions surrounding end-of-life preferences when patients are comfy in an outpatient setting. As the disease state advances additional, integrating care with social employees, pharmacists, and community-based nursing may be critical in enhancing affected person satisfaction with the therapy, enhancing high quality of life, and avoiding coronary heart failure hospitalizations. Equally essential is attention to seasonal influenza vaccinations and periodic pneumococcal vaccines that will obviate non�heart failure hospitalizations in these ill sufferers. Subsequently, heart transplantation exercise within the United States has remained stable at ~2200 per 12 months, but worldwide exercise reported to this registry has decreased somewhat. This obvious decline in numbers may be a result of the reality that reporting is legally mandated within the United States but not elsewhere, and a quantity of other nations have started their very own databases. The donor heart is mostly "harvested" by a separate surgical group, transported from the donor hospital in a bag of iced saline solution, and reanastomosed into the ready recipient in the orthotopic or normal anatomic place. The solely change in surgical technique since this methodology was first described has been a motion in current years to move the right atrial anastomosis again to the extent of the superior and inferior venae cavae to better protect right atrial geometry and forestall atrial arrhythmias. The physiologic responses of the denervated coronary heart to the calls for of exercise are atypical but fairly sufficient for continuation of regular physical exercise. The United States is split geographically into eleven areas for donor coronary heart allocation. A physiologic limit of ~3 h of "ischemic" (out-of-body) time for hearts precludes a national sharing of hearts. This allocation system design is reissued annually and is conscious of input from a big selection of constituencies, together with both donor families and transplantation professionals. The second highest priority is given to patients requiring ongoing inotropic support, however without a pulmonary artery catheter in place. International pointers produced by the American College of Cardiology/American Heart Association, European Society of Cardiology, and National Institute for Health and Clinical Excellence (United Kingdom) differ of their approach to evaluation of evidence and prioritization of remedy. Conversely, remedy unavailable in the United States, similar to ivabradine and levosimendan, is designated as useful in Europe. There can be regional variation in medicine use even after accounting for indication. Patients from South America are likely to have the bottom charges of comorbidities, revascularization, and system use. In contrast, patients from North America have the best comorbidity burden with high revascularization and system use charges. Given geographic differences in baseline traits and clinical outcomes, the generalizability of therapeutic outcomes in sufferers within the United States and Western Europe could require verification. Mallidi Advanced or end-stage coronary heart failure is an increasingly frequent sequela of many kinds of coronary heart illness, as progressively more effective palliation for the earlier levels of heart illness and prevention of sudden demise related to heart disease turn out to be more widely known and employed (Chap. When sufferers with end-stage or refractory heart failure are recognized, the doctor is confronted with the decision of advising compassionate end-of-life care or choosing to suggest extraordinary life-extending measures. For the occasional affected person who is comparatively young and without serious comorbidities, the latter might characterize an affordable choice. Current therapeutic choices are limited to cardiac transplantation (with the option of mechanical cardiac assistance as a "bridge" to transplantation) or everlasting mechanical help of the circulation. Rates were calculated by the Kaplan-Meier technique, which incorporates info from all transplant recipients for whom any follow-up has been offered. Most sufferers who attain what has lately been categorized as stage D, or refractory end-stage coronary heart failure, are appropriately treated with compassionate end-of-life care. The most recent replace reveals survival charges of 83% and 76% 1 and 3 years after transplantation, respectively, or a posttransplantation "half-life" of 10. The quality of life of survivors is usually excellent, with nicely over 90% of patients within the registry returning to normal and unrestricted perform after transplantation. All at present used regimens are nonspecific, providing basic hyporeactivity to overseas antigens quite than donor-specific hyporeactivity and in addition inflicting the attendant, and undesirable, susceptibility to infections and malignancy. Most cardiac transplantation applications presently use a three-drug routine that includes a calcineurin inhibitor (cyclosporine or tacrolimus), an inhibitor of T cell proliferation or differentiation (azathioprine, mycophenolate mofetil, or sirolimus), and a minimal of a brief preliminary course of glucocorticoids.
Purchase imdur 20 mg line
Drug resistance also can arise in herpesviruses however is a much less frequent clinical drawback advanced pain institute treatment center generic imdur 20 mg without a prescription. Smallpox has been eradicated besides as a possible weapon of biological warfare or bioterrorism (Chap anesthesia pain treatment center nj generic imdur 20mg mastercard. New rotavirus vaccines can have a major impact on this leading explanation for gastroenteritis and outstanding reason for childhood demise worldwide groin pain treatment video cheap imdur 40 mg line. Retrovirus integration into the cell genome has been used to functionally substitute the irregular gene in T cells of patients with severe mixed immunodeficiency, thereby restoring immune function. Recombinant poxviruses, adenoviruses, and influenza viruses are also getting used experimentally as vaccine vectors. Viral vectors are being examined experimentally for the expression of cytokines that may enhance immunity in opposition to tumor cells or for the expression of proteins that may enhance the sensitivity of tumor cells to chemotherapy. For improved security, nonreplicating viruses are regularly used in clinical trials. Potential antagonistic events related to virus-mediated gene transfer embrace the induction of inflammatory and antiviral immune responses. Instances of retrovirus-induced human malignances have raised considerations about the security of retroviral gene remedy vectors. The enzyme cleaves terminal sialic acid residues and thus destroys the mobile receptors to which the viral hemagglutinin attaches. Zanamivir and oseltamivir are sialic acid transitionstate analogues and are highly lively and specific inhibitors of the neuraminidases of each influenza A and B viruses. The antineuraminidase activity of the 2 medicine is comparable, though zanamivir has somewhat greater in vitro exercise against influenza B virus. Zanamivir may be lively against sure strains of influenza A virus which are immune to oseltamivir. Both zanamivir and oseltamivir act via competitive and reversible inhibition of the lively website of influenza A and B viral neuraminidases and have comparatively little impact on mammalian cell enzymes. Orally administered oseltamivir has a bioavailability of >60% and a plasma half-life of 7�9 h. Zanamivir has low oral bioavailability and is administered orally through a hand-held inhaler. The toxicities most regularly encountered with orally administered oseltamivir are nausea, gastrointestinal discomfort, and (less commonly) vomiting. Zanamivir is orally inhaled and is mostly properly tolerated, although exacerbations of bronchial asthma could happen. Inhaled zanamivir and orally administered oseltamivir have been effective within the therapy of naturally occurring, uncomplicated influenza A or B in otherwise wholesome adults. Pooled analyses of clinical studies of oseltamivir suggest that treatment may scale back the chance of hospitalizations and of certain respiratory tract problems associated with influenza, and observational research suggest that oseltamivir might scale back mortality charges related to influenza A outbreaks (Chap. Once-daily inhaled zanamivir or once-daily orally administered oseltamivir can present prophylaxis against laboratory-documented influenza A� and influenza B�associated sickness. Resistance to the neuraminidase inhibitors could develop by changes within the viral neuraminidase enzyme, by modifications within the hemagglutinin that make it extra proof against the actions of the neuraminidase, or by each mechanisms. Isolates which are immune to oseltamivir-most commonly by way of the H275Y mutation, which outcomes in a change from histidine to tyrosine at that residue in the neuraminidase-remain delicate to zanamivir. Because the mechanisms of motion of the neuraminidase inhibitors differ from those of the adamantanes (see below), zanamivir and oseltamivir are lively against strains of influenza A virus which may be proof against amantadine and rimantadine. Appropriate use of antiviral brokers against influenza viruses is decided by a information of the resistance patterns of circulating viruses. As of this writing, currently circulating influenza A/H1N1 and H3N2 viruses (2013�2014) have been sensitive to zanamivir and oseltamivir, with a few exceptions for oseltamivir. Viruses replicate intracellularly and sometimes use host cell enzymes, macromolecules, and organelles for synthesis of viral particles. Therefore, helpful antiviral compounds must discriminate between host and viral features with a excessive diploma of specificity; agents without such selectivity are prone to be too toxic for clinical use. Significant progress has also been made within the improvement of laboratory assays to help clinicians in the applicable use of antiviral drugs. Phenotypic and genotypic assays for resistance to antiviral drugs have gotten extra widely obtainable, and correlations of laboratory outcomes with scientific outcomes are being higher defined. Of explicit observe has been the event of extremely sensitive and particular strategies that measure the concentration of virus in blood (virus load) and allow direct evaluation of the antiviral impact of a given drug routine in that host website. Virus load measurements have been useful in recognizing the danger of illness progression in patients with viral infections and in figuring out sufferers for whom antiviral chemotherapy might be of best benefit. As with any in vitro laboratory check, outcomes are highly depending on and certain vary with the laboratory strategies used. Information concerning the pharmacodynamics of antiviral drugs, and particularly the relationship of concentration results to efficacy, has been gradual to develop but can be increasing. However, assays to measure concentrations of antiviral medicine, especially of their lively moieties within cells, are nonetheless primarily analysis procedures not broadly obtainable to clinicians. Thus, there are restricted pointers for adjusting dosages of antiviral agents to maximize antiviral exercise and minimize toxicity. Consequently, medical use of antiviral medicine have to be accompanied by explicit vigilance for unanticipated antagonistic effects. Like that of other infections, the course of viral infections is profoundly affected by interplay between the pathogen and a complex set of host defenses. The presence or absence of preexisting immunity, the power to mount humoral and/or cell-mediated immune responses, and the stimulation of innate immunity are necessary determinants of the end result of viral infections. As with any therapy, the optimum use of antiviral compounds requires a specific and well timed analysis. For some viral infections, corresponding to herpes zoster, the clinical manifestations are so attribute that a diagnosis could be made on scientific grounds alone. Considerable progress has additionally been made in current years within the improvement of such exams, which at the second are broadly available for a quantity of viral infections. Their effectiveness in prevention or remedy of problems is unclear, though some analyses counsel that oseltamivir might scale back the frequency of respiratory tract problems and hospitalizations. Their efficacy in treatment of uncomplicated disease caused by sensitive viruses has been much like that of neuraminidase inhibitors. Prophylaxis must be continued throughout exposure and can be administered simultaneously with inactivated vaccine. Unless the sensitivity of isolates is understood, neither amantadine nor rimantadine is at present really helpful for prophylaxis or therapy. Treatment confers modest clinical benefit when administered inside 24 h of rash onset. Valacyclovir appears to be as effective as acyclovir but can be administered less regularly. Treatment is run during periods when intense immunosuppression is expected-.
Cheap imdur 40mg visa
The main determinants of preload pain burns treatment cheap imdur 40 mg with amex, afterload pain treatment satisfaction scale (ptss) generic imdur 40mg fast delivery, and contractility are proven in Table 265e-2 pain and treatment center greensburg pa generic imdur 40 mg amex. This length offers the optimum configuration for the interaction between the 2 sets of myofilaments. According to this concept, termed length-dependent activation, myofilament sensitivity to Ca2+ is also maximal at the optimum sarcomere length. The latter acts via protein kinase A to stimulate metabolism (left) and phosphorylate the Ca2+ channel protein (right). In isolated coronary heart and heart-lung preparations, the stroke volume varies instantly with the end-diastolic fiber length (preload) and inversely with the arterial resistance (afterload), and as the heart fails-i. The relation between the ventricular end-diastolic strain and the stroke work of the ventricle (the ventricular operate curve) offers a useful definition of the level of contractility of the center within the intact organism. An improve in contractility is accompanied by a shift of the ventricular operate curve upward and to the left (greater stroke work at any stage of ventricular end-diastolic pressure, or decrease end-diastolic volume at any stage of stroke work), whereas a shift downward and to the proper characterizes depression of contractility. The larger cycle is totally intracellular and entails Ca2+ fluxes into and out of the sarcoplasmic reticulum, in addition to Ca2+ binding to and launch from troponin C. The action potential opens plasma membrane Ca2+ channels to enable passive entry of Ca2+ into the cell from the extracellular fluid (arrow A). In the intracellular Ca2+ cycle, passive Ca2+ launch occurs by way of channels in the cisternae (arrow C) and initiates contraction; active Ca2+ uptake by the Ca2+ pump of the sarcotubular network (arrow D) relaxes the guts. Conversely, on the identical aortic stress and ventricular diastolic quantity, the afterload on a hypertrophied ventricle is decrease than of a normal chamber. The aortic stress in turn depends on the peripheral vascular resistance, the bodily characteristics of the arterial tree, and the volume of blood it contains on the onset of ejection. As already famous, elevations in each preload and contractility enhance myocardial fiber shortening, whereas increases in afterload scale back it. The extent of myocardial fiber shortening and left ventricular size determine stroke volume. Increased afterload additionally could outcome from neural and humoral stimuli that happen in response to a fall in cardiac output. Treatment with vasodilators has the other impact; when afterload is lowered, cardiac output rises (Chap. Under normal circumstances, the assorted influences appearing on cardiac performance enumerated above interact in a complex style to maintain cardiac output at a degree applicable to the necessities of the metabolizing tissues. For instance, a reasonable reduction of blood volume or the lack of the atrial contribution to ventricular contraction ordinarily may be sustained without a discount in the cardiac output at relaxation. Under these circumstances, different factors, such as increases in the frequency of adrenergic nerve impulses to the heart, heart fee, and venous tone, will serve as compensatory mechanisms and maintain cardiac output in a traditional particular person. In the intact heart, the afterload could additionally be outlined as the strain developed in the ventricular wall throughout ejection. Hyperventilation, the pumping action of the exercising muscle tissue, and venoconstriction throughout train all augment venous return and hence ventricular filling and preload (Table 265e-2). Vasodilation occurs within the exercising muscle tissue, thus tending to restrict the increase in arterial strain that otherwise would happen as cardiac output rises to ranges as excessive as 5 times larger than basal levels throughout maximal train. This vasodilation in the end permits the achievement of a tremendously elevated cardiac output throughout train at an arterial stress solely reasonably higher than in the resting state. The cardiac output and stroke quantity may be depressed within the presence of heart failure, but not uncommonly, these variables are inside regular limits in this condition. Alternatively, abnormally elevated ventricular end-diastolic volume (normal worth = seventy five ďż˝ 20 mL/m2) or end-systolic quantity (normal value = 25 ďż˝ 7 mL/m2) signifies impairment of left ventricular systolic perform. They provide measurements of end-diastolic and end-systolic volumes, ejection fraction, and systolic shortening fee, and they allow assessment of ventricular filling (see below) in addition to regional contraction and leisure. A limitation of measurements of cardiac output, ejection fraction, and ventricular volumes in assessing cardiac operate is that ventricular loading conditions strongly influence these variables. Thus, a depressed ejection fraction and lowered cardiac output might happen in sufferers with regular ventricular function but decreased preload, as happens in hypovolemia, or with elevated afterload, as occurs in acutely elevated arterial strain. Stroke volume mixed with heart rate determines cardiac output, which, when combined with peripheral vascular resistance, determines arterial strain for tissue perfusion. The characteristics of the arterial system also contribute to afterload, an increase that reduces stroke quantity. The interplay of those components with carotid and aortic arch baroreceptors provides a feedback mechanism to greater medullary and vasomotor cardiac centers and to greater levels within the central nervous system to effect a modulating influence on heart price, peripheral vascular resistance, venous return, and contractility. These two principal sources of acetyl coenzyme A in cardiac muscle range reciprocally. Effects of will increase in preload and afterload on the administration of inotropic agents, hypoxia, and gentle pressure-volume loop. With an increase in cose manufacturing ensuing from glycogenolysis, and afterload, stroke quantity falls (1 2); with an increase in preload, stroke volume rises glucose metabolism to pyruvate (glycolysis). Ventricular stiffness increases with hypertrophy and conditions that infiltrate the ventricle, corresponding to amyloid, or is attributable to an extrinsic constraint. Normally, the rate of influx is more speedy in early diastole than during atrial systole; with delicate to reasonably impaired relaxation, the speed of early diastolic filling declines, whereas the speed of presystolic Increased chamber Chamber stiffness dilation filling rises. With additional impairment of filling, the sample is "pseudonormalized," and early ventricular filling becomes extra rapid as left atrial pressure upstream to the stiff left ventricle rises. Mutations in these genes 265e-11 are liable for some forms of inherited congenital coronary heart disease. Cardiac precursors coalesce to kind a midline heart tube composed of a single cell layer of endocardium surrounded by a single layer of myocardial precursors. The caudal, inflow region of the center tube, which is destined to adopt a more rostral final position, represents the atrial anlagen, whereas the rostral, outflow portion of the tube varieties the truncus arteriosus, which divides to produce the aorta and the proximal pulmonary artery. The linear heart tube undergoes an asymmetric looping course of (the Developmental Biology of the Cardiovascular System the guts is the primary gross evidence of left-right asymmetry in the creating embryo), first organ to kind throughout embryogenesis. Looping is coordinated with chamber specifigrow and undergo advanced morphogenetic modifications. Early pro- cation and ballooning of varied areas of the center tube to produce genitors of the guts arise within very early crescent-shaped fields the presumptive atria and ventricles. These cells, which are derived from regulatory transcription elements that play reiterated roles in cardiac what is called the second heart area, migrate to the center from the ventral pharynx and categorical markers that permit for their identification, including Early heart-forming Neural folds Pericardial Foregut Forming heart Islet-1. Different embryologic origins of areas coelom cells within the right and left ventricles might assist clarify why some forms of congenital and grownup heart diseases affect these regions of the heart to various levels. Cardiac valves First coronary heart subject Second heart subject kind between the atria and the ventricles and between the ventricles and the outflow vessels. The great vessels form as a series of bilaterally symmetric aortic arch arteries that endure asymmetric transforming occasions to type the mature vasculaF ture. Schematic depiction of a transverse part via an early embryo depicts orchestrates this course of. The bilateral heart tubes subsequently required for aortic arch remodeling and migrate to the midline and fuse to kind the linear coronary heart tube.
Best imdur 20 mg
Virus then enters the bloodstream in infected leukocytes (primarily monocytes) pain treatment guidelines 2010 purchase imdur 40mg online, producing the primary viremia that disseminates an infection all through the reticuloendothelial system american pain society treatment guidelines discount imdur 40 mg. Further replication leads to secondary viremia that begins 5�7 days after infection and disseminates measles virus all through the body the pain treatment center of the bluegrass cheap imdur 40 mg free shipping. Spread of measles virus, from preliminary an infection of the respiratory tract through dissemination to the pores and skin. Early nonspecific (innate) immune responses through the prodromal phase include activation of pure killer cells and elevated production of antiviral proteins. The adaptive immune responses include measles virus�specific antibody and cellular responses. The protective efficacy of antibodies to measles virus is illustrated by the immunity conferred to infants from passively acquired maternal antibodies and the protection of exposed, vulnerable people after administration of anti�measles virus immunoglobulin. The first measles virus�specific antibodies produced after infection are of the IgM subtype, with a subsequent change to predominantly IgG1 and IgG4 isotypes. The IgM antibody response is often absent following reexposure or revaccination and serves as a marker of major an infection. The importance of cellular immunity to measles virus is demonstrated by the ability of children with agammaglobulinemia (congenital lack of ability to produce antibodies) to recover totally from measles and the contrasting picture for kids with severe defects in T lymphocyte perform, who usually develop extreme or deadly illness (Chap. The duration of protecting immunity following wild-type measles virus infection is generally thought to be lifelong. However, the extraordinary immune responses induced by measles virus infection are paradoxically associated with depressed responses to unrelated (non�measles virus) antigens, which persist for a quantity of weeks to months past decision of the acute illness. This state of immune suppression enhances susceptibility to secondary infections with micro organism and viruses that cause pneumonia and diarrhea and is responsible for a substantial proportion of measles-related morbidity and deaths. Delayed-type hypersensitivity responses to recall antigens, similar to tuberculin, are suppressed, and cellular and humoral responses to new antigens are impaired. Reactivation of tuberculosis and remission of autoimmune diseases after measles have been described and are attributed to this era of immune suppression. The lesions seem first on the buccal mucosa opposite the decrease molars but rapidly increase in quantity to contain the whole buccal mucosa. The rash of measles begins as erythematous macules behind the ears and on the neck and hairline. Areas of confluent rash appear on the trunk and extremities, and petechiae could additionally be present. The rash fades slowly in the identical order of development because it appeared, often beginning on the third or fourth day after onset. Resolution of the rash may be followed by desquamation, particularly in undernourished children. Because the characteristic rash of measles is a consequence of the mobile immune response, it might not develop in persons with impaired cellular immunity. These individuals have a high case-fatality price and regularly develop giant-cell pneumonitis brought on by measles virus. A severe atypical measles syndrome was observed in recipients of a formalin-inactivated measles vaccine (used in the United States from 1963 to 1967 and in Canada until 1970) who were subsequently exposed to wild-type measles virus. The atypical rash began on the palms and soles and unfold centripetally to the proximal extremities and trunk, sparing the face. The rash was initially erythematous and maculopapular but frequently progressed to vesicular, petechial, or purpuric lesions. The atypical lymphocytosis in infectious mononucleosis contrasts with the leukopenia commonly observed in youngsters with measles. Clinical diagnosis is more difficult (1) during the prodromal illness; (2) when the rash is attenuated by passively acquired antibodies or prior immunization; (3) when the rash is absent or delayed in immunocompromised youngsters or severely undernourished youngsters with impaired cellular immunity; and (4) in areas where the incidence of measles is low and different pathogens are accountable for nearly all of diseases with fever and rash. The detection of measles virus�specific IgM in a single specimen of serum or oral fluid is considered diagnostic of acute an infection, as is a fourfold or greater improve in measles virus�specific IgG antibody levels between acute- and convalescent-phase serum specimens. Primary infection within the immunocompetent host results in antibodies that are detectable inside 1�3 days of rash onset and reach peak ranges in 2�4 weeks. Measles virus�specific IgM antibodies will not be detectable until 4�5 days or extra after rash onset and usually fall to undetectable levels inside 4�8 weeks of rash onset. The diagnosis requires laboratory affirmation besides during large outbreaks in which an epidemiologic hyperlink to a confirmed case could be established. Care is largely supportive and consists of the administration of vitamin A and antibiotics (see "Treatment," below). Complications of measles, together with secondary bacterial infections and encephalitis, could occur after acute illness and require cautious monitoring, significantly in immunocompromised persons. Fever and malaise starting ~10 days after exposure are adopted by cough, coryza, and conjunctivitis. Measles can be diagnosed by isolation of the virus in cell culture from respiratory secretions, nasopharyngeal or conjunctival swabs, blood, or urine. Direct detection of large cells in respiratory secretions, urine, or tissue obtained by biopsy provides another methodology of diagnosis. Extremely delicate and particular, this assay may also allow identification and characterization of measles virus genotypes for molecular epidemiologic research and might distinguish wildtype from vaccine virus strains. Treatment consists of basic supportive measures, corresponding to hydration and administration of antipyretic brokers. Streptococcus pneumoniae and Haemophilus influenzae sort b are widespread causes of bacterial pneumonia following measles; vaccines towards these pathogens most likely decrease the incidence of secondary bacterial infections following measles. Vitamin A is efficient for the therapy of measles and can markedly reduce charges of morbidity and mortality. A third dose is really helpful 2�4 weeks later for youngsters with evidence of vitamin A deficiency. Acute laryngotracheobronchitis (croup) can occur during measles and should result in airway obstruction, particularly in younger kids. Most issues of measles result from secondary bacterial infections of the respiratory tract which might be attributable to a state of immune suppression lasting for a number of weeks to months after acute measles. Recurrence of fever or failure of fever to subside with the rash suggests secondary bacterial infection. Postmeasles encephalomyelitis complicates ~1 in one thousand cases, affecting primarily older youngsters and adults. Encephalomyelitis happens within 2 weeks of rash onset and is characterised by fever, seizures, and a big selection of neurologic abnormalities. The finding of periventricular demyelination, the induction of immune responses to myelin primary protein, and the absence of measles virus in the brain recommend that postmeasles encephalomyelitis is an autoimmune dysfunction triggered by measles virus infection. Measles case-fatality proportions range with the average age of an infection, the nutritional and immunologic status of the population, measles vaccine protection, and access to health care. Among beforehand vaccinated individuals who do turn out to be infected, illness is much less extreme and mortality charges are considerably decrease.
Populus canadensis (Poplar). Imdur.
- Cough, minor skin injuries, hemorrhoids, frostbite, and sunburn.
- What is Poplar?
- Are there safety concerns?
- Dosing considerations for Poplar.
- How does Poplar work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96270
Imdur 20 mg line
Some very primary analysis knowledge point to the early use of anti-inflammatory preparations joint and pain treatment center thousand oaks order imdur 40 mg visa. Denuded areas ought to be irrigated three or four times daily with saline advanced pain institute treatment center cheap 40 mg imdur with amex, other sterile 262e-4 solutions pain treatment after root canal purchase imdur 40mg free shipping, or soapy water and then liberally coated with the topical antibiotic of selection, similar to silver sulfadiazine, mafenide acetate, or triple antibiotic ointment to a thickness of 1�2 mm. Some physicians advocate sterile needle drainage of huge blisters, with collapsing of the blister roof to type a sterile dressing. Systemic analgesics must be used liberally, notably earlier than manipulation of the affected person. Overly rigorous hydration appears to have precipitated pulmonary edema in a couple of Iranian casualties despatched to European hospitals. Conjunctival irritation from a low-vapor publicity responds to any of a selection of out there ophthalmic solutions after the eyes are irrigated completely. A topical antibiotic applied a quantity of occasions a day reduces the incidence and severity of an infection. Animal laboratory information mirror outstanding outcomes with early utility of commercially available topical antibiotic/glucocorticoid ophthalmologic ointments. Petroleum jelly or a similar substance ought to be applied regularly to the perimeters of the eyelids to prevent them from sticking together. Topical analgesics, although of limited value, could also be useful initially if blepharospasm is simply too extreme to allow an enough examination. A productive cough and dyspnea accompanied by fever and leukocytosis occurring within 12�24 h are indicative of chemical pneumonitis. The clinician must resist the urge to use prophylactic antibiotics for this process. Infection usually occurs on the third to fifth day and is signaled by elevated fever, a pulmonary infiltrate, and increased sputum production with a change in colour. Intubation could also be essential if laryngeal spasm or edema makes breathing troublesome or becomes life-threatening. Intubation permits higher air flow and facilitates suctioning of necrotic and inflammatory debris. Pseudomembrane formation might require fiberoptic bronchoscopy for suctioning of necrotic debris. There is little evidence that the routine use of glucocorticoids is beneficial besides for added relief of bronchospasm. In the Iran�Iraq war, a white blood cell rely of 200/L often resulted in dying of the affected person. Sterilization of the gut by nonabsorbable antibiotics must be thought-about to scale back the potential for sepsis from enteric organisms. Granulocyte colony-stimulating issue produced a 50% discount within the time required for bone marrow restoration in nonhuman primates exposed to sulfur mustard. Medication for nausea and vomiting may be essential for gastrointestinal unwanted effects. Lymphopenia precedes basic leukopenia by a day or extra and may be a helpful clinical tip-off to impending leukopenia. Some examples embody (1) the demonstration of a reduction by up to 75% of irritation and tissue harm within the mouse ear swelling check by vanilloid compounds and (2) the demonstration of 50�60% safety by N-acetylcysteine within the technology of free radicals within guinea pig lung exposed to mustard. In many cases, the demonstration of safety depends on the supply of sufficient amounts of medicine with sufficient half-lives. Strategies to improve bioavailability include attachment of polyethylene glycol to the antioxidant drug/enzyme and/or supply of the drug/enzyme in a liposome. They work by inhibition of tissue synaptic acetylcholinesterase, creating an acute cholinergic crisis. Death ensues due to respiratory melancholy and might happen inside seconds to minutes. The nerve brokers tabun and sarin were first used on the battlefield by Iraq against Iran through the first Persian Gulf War (1984�1987). In 1994 and 1995, the Japanese cult Aum Shinrikyo used sarin in two terrorist assaults in Matsumoto and Tokyo. All the nerve brokers are organophosphorus compounds, that are liquid at commonplace temperature and pressure. The "G" brokers evaporate at in regards to the rate of water, except for cyclosarin, which is oily and thus probably will have evaporated inside 24 h after deposition on the ground. In the Tokyo subway assault during which sarin was used, one hundred pc of the symptomatic sufferers inhaled sarin vapor that spilled out on the floor of the subway cars. Mechanism Acetylcholinesterase inhibition accounts for the most important life-threatening effects of nerve agent poisoning. The efficacy of antidotal remedy in the reversal of this inhibition proves that this is the primary poisonous action of these poisons. At cholinergic synapses, acetylcholinesterase, bound to the postsynaptic membrane, functions as a turn-off change to regulate cholinergic transmission. Inhibition of acetylcholinesterases causes the launched neurotransmitter, acetylcholine, to accumulate abnormally. End-organ overstimulation, which is acknowledged by clinicians as a cholinergic disaster, ensues. Clinical Features Clinical effects of nerve agent exposure are identical for vapor and liquid exposure routes if the dose is sufficiently giant. Exposure of a affected person to nerve agent vapor, by far the extra likely route of publicity in both battlefield and terrorist eventualities, will cause cholinergic symptoms within the order in which the toxin encounters cholinergic synapses. Nerve agent vapor easily crosses the cornea, interacts with these synapses, and produces miosis, described by Tokyo subway victims as "the world going black. As a outcome, acetylcholine, which normally is launched from presynaptic membrane however then is degraded, accumulates, and this leads to organ overstimulation and cholinergic disaster. Exocrine glands within the nose, mouth, and pharynx are subsequent uncovered to the vapor, and cholinergic overload here causes elevated secretions, rhinorrhea, extra salivation, and drooling. Toxin then interacts with exocrine glands in the higher airway, inflicting bronchorrhea, and with bronchial clean muscle, inflicting bronchospasm. Once the victim has inhaled, vapor can passively cross the alveolarcapillary membrane, enter the bloodstream, and incidentally and asymptomatically inhibit circulating cholinesterases, significantly free butyrylcholinesterase and erythrocyte acetylcholinesterase, each of which may be assayed. Unfortunately, the results of this assay may not be simply interpretable with no baseline, since cholinesterase ranges vary enormously between individuals and over time in a person, wholesome patient. Usually the first organ system to turn out to be symptomatic from bloodborne nerve agent publicity is the gastrointestinal tract, where cholinergic overload causes stomach cramping and pain, nausea, vomiting, and diarrhea. After the gastrointestinal tract becomes involved, nerve agents will have an result on the heart, distant exocrine glands, muscles, and mind. Remote exocrine exercise will embody oversecretion within the salivary, nasal, respiratory, and sweat glands-the affected person shall be "wet all over. In the brain, because the cholinergic system is so widely distributed, bloodborne nerve brokers will, in enough doses, cause speedy lack of consciousness, seizures, and central apnea resulting in dying within minutes. If standing epilepticus persists, neuronal demise and permanent brain dysfunction may happen. Even in gentle nerve-agent intoxication, sufferers may recover however may experience weeks of irritability, sleep disturbance, and nonspecific neurobehavioral manifestations.
Discount 40 mg imdur fast delivery
All patients beginning remedy with ethambutol should have a baseline test for visual acuity unifour pain treatment center purchase imdur 40 mg overnight delivery, visual fields cape fear pain treatment center imdur 20 mg overnight delivery, and color imaginative and prescient and will undergo an examination of the optic fundus kneecap pain treatment buy discount imdur 40mg line. Visual acuity and colour vision should be monitored month-to-month or much less usually as wanted. Cessation of ethambutol in response to early symptoms of ocular toxicity normally results in reversal of the deficit inside several months. Some experts assume that supplementation with hydroxocobalamin (vitamin B12) is useful for patients with ethambutol-related ocular toxicity. Its administration for the primary 2 months of therapy with rifampin and isoniazid permits treatment duration to be shortened from 9 months to 6 months and decreases rates of relapse. The drug is extra lively in opposition to slowly replicating organisms than in opposition to actively replicating organisms. PharMacology anD Dosing Pyrazinamide is nicely absorbed after oral administration, with peak serum concentrations of 20�60 g/mL at 1�2 h after ingestion of the beneficial grownup daily dose of 15�30 mg/kg (maximum, 2 g/d). A excessive proportion of pyrazinamide and its metabolites (~70%) is excreted in the urine. The dosage have to be adjusted in accordance with the level of renal function in sufferers with lowered creatinine clearance. Hyperuricemia is a standard opposed impact of pyrazinamide remedy that usually can be managed conservatively. There is some controversy as to the clinical significance of in vitro pyrazinamide resistance. Protease inhibitors could trigger significant will increase in rifabutin levels by way of inhibition of hepatic metabolism. PharMacology Like rifampin, rifabutin is lipophilic and is absorbed quickly after oral administration, reaching peak serum levels 2�4 h after ingestion. Rifabutin distributes greatest to tissues, reaching levels 5�10 occasions higher than those in plasma. Unlike rifampin, rifabutin and its metabolites are partially cleared by the hepatic microsomal system. Clarithromycin (but not azithromycin) and fluconazole seem to improve rifabutin ranges by inhibiting hepatic metabolism. The most typical adverse occasions are gastrointestinal; different reactions embrace rash, headache, asthenia, chest ache, myalgia, and insomnia. Less frequent antagonistic reactions embody fever, chills, a flulike syndrome, anterior uveitis, hepatitis, Clostridium difficile� associated diarrhea, a diffuse polymyalgia syndrome, and yellow pores and skin discoloration ("pseudo-jaundice"). Laboratory abnormalities include neutropenia, leukopenia, thrombocytopenia, and elevated levels of liver enzymes. Rifapentine Rifapentine is a semisynthetic cyclopentyl rifamycin, sharing a mechanism of action with rifampin. Rifapentine is lipophilic and has a prolonged half-life that permits weekly or twice-weekly dosing. Therefore, this drug is the subject of intensive clinical investigation aimed toward determining optimal dosing and frequency of administration. When administered in these particular circumstances, rifapentine (10 mg/kg, up to 600 mg) is given as soon as weekly with isoniazid. Although the speed of permanent drug discontinuation because of adverse occasions was larger with rifapentine/ isoniazid, this routine had the next therapy completion price than day by day isoniazid on this examine. After oral administration, rifapentine reaches peak serum concentrations in 5�6 h and achieves a gentle state in 10 days. The half-life of rifapentine and its active metabolite, 25-desacetyl rifapentine, is ~13 h. Rifapentine is teratogenic in animal models and is comparatively contraindicated in pregnancy. Derived from Streptomyces griseus, streptomycin is bactericidal towards dividing M. In developed nations, streptomycin is used sometimes because of its toxicity, the inconvenience of injections, and drug resistance. MechanisM of action Streptomycin inhibits protein synthesis by binding at a website on the 30S mycobacterial ribosome. PharMacology anD Dosing Serum ranges of streptomycin peak at 25�45 g/mL after a 1-g dose. For sufferers 60 years of age, 10 mg/kg is the really helpful daily dose, with a maximum of 750 mg/d. Because streptomycin is eliminated nearly solely by the kidneys, its use in sufferers with renal impairment ought to be prevented or implemented with caution, with decrease doses and fewer frequent administration. Ototoxicity (primarily vestibulotoxicity), neuropathy, and renal toxicity are the most common and probably the most serious. Renal toxicity, often manifested as nonoliguric renal failure, is less frequent with streptomycin than with different incessantly used aminoglycosides, corresponding to gentamicin. Manifestations of vestibular toxicity include lack of stability, vertigo, and tinnitus. Patients receiving streptomycin must be monitored fastidiously for these adverse results, undergoing audiometry at baseline and month-to-month thereafter. However, low-level resistance, which is seen in about one-third of resistant isolates, has no related resistance mutation. A gene (gidB) that confers low-level resistance to streptomycin has just lately been recognized. The later-generation fluoroquinolones levofloxacin and moxifloxacin are essentially the most lively in opposition to M. Fluoroquinolones are additionally considered safe options for patients who develop treatment-limiting opposed effects because of first-line agents. The optimal dose of levofloxacin for this indication is being actively studied, however doses of no less than 750 mg are commonly used. The fluoroquinolones are properly absorbed orally, reach high serum ranges, and distribute well into physique tissues and fluids. Their absorption is decreased by co-ingestion with products containing multivalent cations, similar to antacids. Mycobacterial resistance can develop quickly when a fluoroquinolone is inadvertently administered alone. Empirical fluoroquinolone remedy for presumed community-acquired pneumonia is associated with elevated fluoroquinolone resistance in M. A dose of 15 mg/kg per day is given 5 to seven occasions per week (maximal day by day dose, 1 g) and results in peak blood ranges of 20�40 g/mL. The dosage could additionally be reduced to 1 g two or three times per week 2�4 months after mycobacterial cultures become adverse. For people 60 years of age, the dose should be decreased to 10 mg/kg per day (maximal day by day dose, 750 mg). For sufferers with renal insufficiency, the drug ought to be given intermittently and at lower dosage (12�15 mg/kg two or 3 times per week). Resistance to capreomycin is related to mutations that inactivate a ribosomal methylase (tlyA) or that encode genes for the 16S ribosomal subunit (rrs). Cross-resistance to kanamycin and amikacin is common with rrs however not all the time with tylA mutations.
Generic imdur 40mg with visa
At 2 years pain in testicles treatment cheap 20 mg imdur amex, there was no distinction in major and the potential for intervening unnecessarily jaw pain tmj treatment purchase imdur 40mg. Most common stress imaging strategies in technique is determined by availability and local experience pain treatment lung cancer buy imdur 20 mg on line. In contemplating the potential clinical software of imaging modalities, the proof supporting the position of Rest evaluation of ischemia versus anatomy have to be considered. In such sufferers, a follow-up stress check is often required to determine the possible want of revascularization. There are also necessary differences in the effectiveness of imaging tests in these patients. Patients with prior coronary artery bypass grafting are a very heterogeneous group with respect to the anatomic foundation of ischemia and its implications for subsequent morbidity and mortality. If an anatomic strategy is indicated, direct referral to invasive angiography is preferred. In these with abnormal stress imaging studies, the degree of abnormality relates to posttest risk. In addition, stress imaging approaches can localize and quantify the magnitude of ischemia (especially with perfusion imaging), thereby helping in planning targeted revascularization procedures. Strategies used within the analysis of these sufferers include novel cardiac biomarkers. In selected patients, stress testing with or with out imaging could also be used for further risk stratification. Stress echocardiography and radionuclide imaging are among the most frequently used imaging approaches in these sufferers. The relative strengths and weaknesses of those testing options have been mentioned above. Overall, there were no deaths and only a few myocardial infarctions without differences between the teams. Taken together, the obtainable information clearly counsel that not all patients presenting with acute chest pain require specialized imaging testing. Patients with very low medical threat and unfavorable biomarkers (especially high-sensitivity troponin assays) may be safely triaged. The use of imaging tests in patients with low-intermediate threat must be carefully considered, particularly given the trade-offs mentioned above. In addition, echocardiography is probably the most costeffective screening method for valvular coronary heart illness. Echocardiography can be utilized to assess both regurgitant and stenotic lesions of any of the cardiac valves. Typical indications for echocardiography to assess valvular heart disease embody cardiac murmurs recognized on physical examination, symptoms of breathlessness that will symbolize valvular heart illness, syncope or presyncope, and preoperative exams in sufferers present process bypass surgical procedure. A commonplace echocardiographic examination ought to embrace qualitative and quantitative assessment of all valves no matter indication and will serve as an enough screening take a look at for vital valvular disease. The morphology of valvular structures offers helpful information relating to the etiology and severity of valvular disease. For instance, two-dimensional imaging assessment of the aortic valve can establish the number of leaflets, decide whether the valve is bicuspid or tricuspid, and determine the severity of calcification and diploma of leaflet excursion. Similarly, the classic look of a rheumatic mitral valve is extremely useful in determining the etiology of mitral stenosis, and mitral valve prolapse can be instantly identified without even the necessity for Doppler-based quantification. For example, when Doppler echocardiography is used to assess the maximal velocity across a stenotic aortic valve, this calculation will provide an correct measure of the instantaneous gradient throughout the valve. This gradient will be greater than the mean gradient, as nicely as greater than that peakto-peak gradient obtained at cardiac catheterization. This gradient depends on both the diploma of stenosis and the contractile function of the left ventricle. Patients with significant left ventricular dysfunction might have extreme aortic stenosis however might be unable to generate a high gradient across the valve because generated pressure within the left ventricle might be diminished. Assessment of stenotic valves typically requires estimation of both the pressure gradient across the valve and the valve area. Pressure gradient is estimated through direct software of the Bernoulli principle, and the formulation p = 4v2 is often adequate to estimate the gradient across the valve. Several strategies can be used to estimate valve areas, including the continuity principle based on the precept of conservation of mass. For instance, for assessment of the aortic valve area, we measure the flow in the region of the left ventricular outflow tract and the cross-sectional area in this region, the product of which ought to be equal to the flow throughout the stenotic aortic valve and its cross-sectional space. Estimation of the mitral valve space in sufferers with suspected mitral stenosis can also be performed in numerous methods, together with planimetry of the valve instantly, estimation with continuity methods, or essentially the most generally used pressure half-time methodology, by which the stenosis severity is estimated by the time it takes for the pressure-estimated from velocity by the Bernoulli equation-to attain half of its original worth throughout mitral inflow. For instance, prolapse of the mitral valve leaflets-and to a lesser extent, the aortic valve leaflets-can be easily visualized with two-dimensional echocardiography. In common, valvular regurgitation can be brought on by abnormalities of the valve leaflets themselves or abnormalities of the annulus and supporting constructions, and these can normally be distinguished visually on transthoracic echocardiography (see dialogue below). Quantification of valvular regurgitation is tougher with echocardiography than quantification of valvular stenoses. Doppler-based methods are best suited to assess blood velocities rather than volumetric move. The most widely used approach for assessing the severity of valvular regurgitation is color circulate Doppler estimation, which is qualitative. Assessment of Aortic Stenosis Aortic stenosis, one of the common types of valvular coronary heart illness, most often happens due to gradual progression of valvular calcification in each normal and congenitally abnormal valves. Echocardiographic evaluation typically begins with visual inspection of the valve, usually in the parasternal long-axis and short-axis views. The regular aortic valve consists of three leaflets or cusps: the right coronary, the left coronary, and the noncoronary cusps. Abnormalities of cusp development are a few of the most typical congenital coronary heart anomalies, the commonest of which is bicuspid aortic valve, with two opening leaflets quite than three. The aortic valve can be visualized on echocardiography, although generally it could be troublesome to distinguish true bicuspid aortic valve from variants, together with the presence of a vestigial commissure (raphe). Echocardiography is the imaging modality of choice both aortic stenosis and aortic insufficiency. As mentioned above, the diploma of aortic stenosis is assessed by for long-term surveillance. Patients with average aortic stenosis or greater generally have Assessment of Aortic Regurgitation Assessment of aortic regurgitation peak instantaneous velocities of three. Because stress gradients throughout the aortic valve can valve, the most common of which is bicuspid aortic valve. However, Congenital abnormalities of the aortic leaflets, corresponding to bicuspid aortic analysis of the affected person with so-called low-flow or low-gradient aortic valve, are widespread causes of aortic insufficiency. Dilatation of the aorstenosis could be difficult and can typically require provocative tic root, as occurs in sufferers with hypertension and different disorders in testing such as dobutamine echocardiography. Hypertrophic cardiomyopathy these measures are often used to resolve the need for valve surgical procedure. Semiquantitative visual assessment of aortic regurgitant because the valve leaflets could be seen opening during systole. The membranes can behave very similarly to leaflet aortic stenosis, and jet diameter as a ratio of the left ventricular outflow tract diameter the membranes themselves can be very skinny and troublesome to visualize, proximal to the valve represents one of the most reliable indices of although the presence of a murmur, a gradient throughout the valve with severity and correlates properly with angiographic assessment.
References
- Kramer LD, Locke GE, Ogunyemi A, et al. Neonatal cocainerelated seizures. J Child Neurol 1990;5:60.
- Thompson GN, Walter JH, Bresson JL, et al. Sources of propionate in inborn errors of metabolism. Metabolism 1990;39:1133.
- Szyfelbein WM, Ross JS. Carcinoids, atypical carcinoids and small-cell carcinomas of the lung: differential diagnosis of fine-needle aspiration biopsy specimens. Diagn Cytopathol 1988;4:1-8.
- Mitake M, Nakazawa S, Naitoh Y, et al. Endoscopic ultrasonography in diagnosis of the extent of gallbladder carcinoma. Gastrointest Endosc. 1990;36(6):562-566.
- Casale P, Grady RW, Joyner BD, et al: Comparison of dismembered and nondismembered laparoscopic pyeloplasty in the pediatric patient, J Endourol 18(9):875n878, 2004.
- Morelli V, Naquin C, Weaver V. Alternative therapies for traditional disease states: osteoarthritis. Am Fam Physician 2003; 67(2):339-44.
- Kanika ND, Chang J, Tong Y, et al: Oxidative stress status accompanying diabetic bladder cystopathy results in the activation of protein degradation pathways, BJU Int 107:1676n1684, 2011.
- Mouzakes J, Koltai PJ. The biology of pediatric facial fractures. Facial Plast Surg Clin North Am 1998;6:487-493.