

Actoplus Met
Tristi W. Muir, MD
- Director, Division of Female Pelvic Medicine and Reconstructive Surgery,
- University of Texas Medical Branch, Galveston, Texas
Actoplus Met dosages: 500 mg
Actoplus Met packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Order 500mg actoplus met mastercard
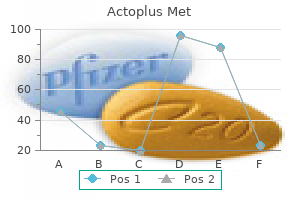
Multidrug-resistant gram-negative bacilli have additionally emerged as a serious threat metabolic disease associates erie pa discount 500 mg actoplus met free shipping, together with multidrug-resistant P test zu diabetes order actoplus met 500 mg on line. For other resistant bacteria diabetic meal plan purchase actoplus met 500mg with visa, similar to penicillin-resistant pneumococci, multiple resistance genes must be cobbled collectively in a selected, exacting sequence, which can take years to evolve, emerge, and unfold. Antibiotic pressures present the necessary Darwinian forces that amplify these genetic adjustments. In some situations, genetic linkage of resistance mechanisms to unrelated classes of antimicrobials results in the capability of heavy use of 1 drug class to select for resistance to a unique class. For instance, use of trimethoprim-sulfamethoxazole has been associated statistically with the emergence of ceftazidimeresistant E. A giant proportion of extended-spectrum -lactamase�producing gram-negative bacilli are additionally proof against fluoroquinolones. First, active surveillance for resistant micro organism is essential to present an understanding of local issues and wishes. To support surveillance and treatment, cultures have to be obtained from suspected sites of an infection before empiric antibiotic remedy is initiated. Aggressive hand hygiene campaigns, with adherence monitoring and feedback of ward and even individual outcomes, could achieve compliance charges as high as 70%. Response to this drawback has been to encourage "common gloving," along with wider use of alcohol-based hand rubs (a "belt-and-suspender" approach) to bridge the hole left by incomplete consideration to hand hygiene even in one of the best of circumstances. The major objective of antimicrobial stewardship is to optimize clinical outcomes whereas minimizing unintended consequences of antimicrobial use, such as toxicity, emergence of resistance, and C. Both antimicrobial stewardship and a comprehensive infection management program are important to limiting the emergence and transmission of antimicrobial-resistant pathogens. A complete evidence-based stewardship program to combat antimicrobial resistance is usually a multifaceted, multidisciplinary program; the scale and complexity of the administration group and the precise measures applied to optimize prescribing differ on the basis of local antimicrobial use patterns, resistance tendencies, and available sources. The two core methods that present the foundation for a successful antimicrobial stewardship program are (1) audits, with intervention and feedback, and (2) formulary restriction and preauthorization. Physicians in the intervention group implemented 85% of the ideas they acquired, which resulted in 1. Effective auditing with intervention and feedback can be undertaken most simply with automated computer surveillance of antimicrobial use, permitting the targeting of particular models the place the problems are greatest. Formulary restriction and preauthorization necessities for specific agents are now widespread in most hospitals. Antimicrobial restriction is unequivocally the simplest method of controlling antimicrobial use. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for growing an institutional program to improve antimicrobial stewardship. Furthermore, restricting the utilization of a single drug to cut back antimicrobial resistance may be ineffective because cross-resistance in bacterial species to a couple of class of antimicrobials is the rule in nosocomial organisms. One or both of the core strategies-audits with intervention and formulary restriction-should be adopted and supplemented by shut collaboration of an antimicrobial stewardship team, infection management personnel, health care providers, and hospital administration. Beyond the 2 core mechanisms of antimicrobial stewardship, other components that should be incorporated into an institutional antimicrobial stewardship program embody education of health care providers; nonetheless, passive academic efforts, such as conference presentations, teaching periods, and provision of tips, are solely marginally efficient in the absence of different lively interventions. Guidelines tailored to native antimicrobial resistance patterns and antimicrobial use tendencies might have extra impact than a generic clinical pathway. Finally, technologies that offer rapid identification of organisms in blood cultures are a promising new application that has improved time to escalation of antimicrobial remedy, and likewise de-escalation of antimicrobial remedy however solely with involvement of the antimicrobial stewardship group (see"Role of the Microbiology Laboratory"). Studies have shown reductions in antimicrobial usage from 22% to 36%, with annual savings of $200,000 to $900,000 in bigger instructing hospitals and neighborhood hospitals. Guidelines from the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America present detailed recommendations for growing institutional applications of antimicrobial stewardship, which are summarized in Table forty seven. This novel therapy relies on the premise that the higher respiratory tract flora exists in a continuum with the gastrointestinal flora and that these mucosal microorganisms make up the most important reservoir of pathogens inflicting pneumonia and heaps of different nosocomial infections, especially in mechanically ventilated sufferers. Studies cited in table (column 1) may be discovered within the complete listing of references for this chapter offered on-line. Preemptive Barrier Isolation Having fewer sufferers in a room, bettering the facilities for handwashing, and utilizing cohort nursing. Among children who have been isolated, the interval before the primary infection was considerably longer (median, 20 vs. Unannounced monitoring showed that kids in each group were touched and dealt with comparably often by hospital personnel and households. Studies cited (by primary author) in desk may be discovered within the full listing of references for this chapter provided on-line. Studies also wants to decide the relative importance of wearing a gown, as compared with sporting gloves alone. Patients with prolonged severe granulocytopenia or those that are receiving high dosages of corticosteroids, often as a part of immunosuppressive regimens to prevent transplant rejection, are in danger for invasive pulmonary an infection brought on by Aspergillus species, mucormycosis, and other filamentous airborne fungi, which is related to a high mortality rate. Approach to a Nosocomial Epidemic See the net complement for Approach to a Nosocomial Epidemic. If an epidemic is suspected, the epidemiologic approach should be methodical and thorough but expeditious, directed toward establishing the bona fide nature of the putative epidemic infections. Control measures are predicated on correct delineation of the epidemiology of the epidemic pathogen. Each hospital, through its an infection management committee, must be prepared administratively to conduct an investigation and implement wanted control measures. During a 2-week period in late March 1985, three sufferers in a university hospital developed main nosocomial bacteremia with an analogous nonfermentative gram-negative bacillus. The bloodstream pathogen in every case was shown to be Pseudomonas pickettii biovariant 1. Molecular subtyping by restriction enzyme digestion and pulsed-field electrophoresis to delineate restriction polymorphism patterns showed all six isolates to be the clonal. All three septic sufferers had had a number of optimistic blood cultures and had been clinically in septic shock. In the hospital on the time, fentanyl was used [only within the working rooms as a half of balanced anesthesia]. Each day, one of the technicians delivered enough pre-drawn syringes to the operating rooms]to meet the wants of the cases being accomplished that day. Cultures of pre-drawn fentanyl in syringes in the central pharmacy, prompted by the findings of the case-control examine, confirmed that 20/50 (40%) 30-mL syringes sampled were contaminated by P. Extensive culturing inside the central pharmacy was unfavorable for proof of environmental contamination by P. A second case-control study advised strongly that the epidemic was attributable to theft of fentanyl from 30-mL syringes by one pharmacy staff member and alternative by distilled water that the person thought was sterile however which, unfortunately, was contaminated by P. The pharmacy member resigned early within the investigation and not works in the hospital. This outbreak illustrates the ability of genetic subtyping155 and case-control analyses to determine the trigger of an epidemic. Remaining products ought to be quarantined and retained for evaluation by the general public well being authorities. Isolates from blood or intravenous fluid of six particular cases (March 1985) have been obtainable for reconfirmation and subtyping as P. E2 pickettii Variable Age, imply (years) Duration of surgical procedure, imply (h) TypeofSurgery Cardiovascular General Intravenous Fluids Lactated Ringer resolution Dextrose in Ringer lactate Salinesolution0.
Order actoplus met 500 mg without prescription
Mechanistic and pharmacologic features of standing epilepticus and its therapy with new antiepileptic medicine definition of diabetes type 2 generic actoplus met 500mg on line. Intensive care for mind damage after cardiac arrest: therapeutic hypothermia and associated neuroprotective methods diabetes test online symptom cheap actoplus met 500mg without a prescription. Randomized clinical trial of the efficacy of antiepileptic medicine in decreasing the danger of relapse after a primary unprovoked tonic-clonic seizure blood glucose explained generic actoplus met 500 mg with visa. Phenytoin publicity is related to practical and cognitive disability after subarachnoid hemorrhage. Prospective, randomized, single-blinded comparative trial of intravenous levetiracetam versus phenytoin for seizure prophylaxis. The affect of diazepam or lorazepam on the frequency of endotracheal intubation in childhood status epilepticus. A comparability of lorazepam, diazepam, and placebo for the remedy of out-of-hospital standing epilepticus. Incidence and clinical consequence of the purple glove syndrome in patients receiving intravenous phenytoin. Treatment of standing epilepticus: a prospective comparability of diazepam and phenytoin versus phenobarbital and elective phenytoin. Prognostic elements of pentobarbital remedy for refractory generalized standing epilepticus. High-dose pentobarbital treatment of refractory standing epilepticus: a meta-analysis of revealed studies. Safety of speedy intravenous infusion of valproate loading doses in epilepsy sufferers. Intravenous valproate related to important hypotension in the therapy of status epilepticus. Mitochondrial diseases symbolize a danger issue for valproate-induced fulminant liver failure. Meropenem-valproic acid interaction in sufferers with cefepime-associated standing epilepticus. Intravenous lacosamide�an efficient add-on remedy of refractory status epilepticus. Efficacy of intravenous lacosamide as an add-on treatment in refractory status epilepticus: a multicentric prospective examine. Neurologic recovery after therapeutic hypothermia in patients with post-cardiac arrest myoclonus. Neurologic prognosis in cardiac arrest sufferers treated with therapeutic hypothermia. A 69-year-old man presents to the emergency department after three witnessed generalized tonic-clonic seizures that began 1 hour before arrival. Which of the next medicines must be the first-line therapy for this patient The patient has had three seizures with no enchancment in his mentation, meeting criteria for status epilepticus. The Veterans Affairs Status Epilepticus Cooperative Study confirmed lorazepam to be the most effective agent in terminating seizures compared with diazepam or phenytoin. The affected person required intubation on presentation for hypoxemic respiratory failure. She has obtained 3 days of antibiotics with decision of fevers, leukocytosis, and she has now been successfully weaned from vasopressor support. On hospital day 3 she has not yet awakened after sedatives have been discontinued for more than 24 hours. Antibiotics associated with lowering of seizure threshold embrace penicillins, carbapenems, and cefepime. She is otherwise wholesome, but she began experiencing persona modifications 2 weeks before presentation. The management of serious brain trauma requires specialty teams consisting of experienced neurosurgeons, traumatologists, intensivists, and neurointensivists working collectively in a devoted unit equipped and staffed to optimally take care of these sufferers. This strategy results in targeted conclusions that might be limited by examine design and are, subsequently, rigorously worded to reflect the precise methodology of the research used to support a specific suggestion. Nearly a third of all traumatic deaths in the United States contain a head damage. The search for neuroprotective and neuroregenerative therapies that can consistently stop or reverse the devastating cascade of events that results in irreparable brain damage stays for future investigators as of this writing. Key to optimizing clinical outcomes has been the recognition that the time from harm to surgical procedure have to be as brief as attainable to reduce the secondary manifestations of great brain trauma in sufferers with surgical lesions. The operating room is where sufferers with significant mass impact and shift are initially managed. Level of consciousness is certainly one of the most essential neurologic concerns in managing a affected person with a head harm. Neurosurgical sufferers typically have an alteration in stage of consciousness from either brainstem or bilateral cerebral hemispheric involvement. Many scientific evaluation instruments are available to be used in the crucial care setting. It is predicated on eye opening (1�4 points), verbal response (1�5 points), and motor response (1�6 points) (Table sixty three. A affected person with a normal stage of consciousness should have the best possible rating of 15. Commonly, an intubated patient will get a 1 for verbal response and is assigned 1T (for Tube) for the verbal score. Therefore you will need to notice the shortcoming of this system in evaluating sufferers with dementia or aphasia. Plain x-ray movies of the skull are rarely indicated as a screening study for patients with head injuries. Using these 4 predictors, quite a few investigators have used statistical modeling techniques to predict as a lot as 80% or more of outcomes. The authors chose to add +1 to make the grading numerically according to the grading of the motor score of the Glasgow Coma Scale and with the Marshall computed tomography classification. Located in the brainstem, the reticular activating system is what allows a meaningful, awake condition; whether it is destroyed, the patient might be in a vegetative state. The surgical management of patients with head accidents is usually driven by the presence of pathologic plenty (hematomas) in anatomic spaces. In most circumstances of head injury seen in neurosurgical apply, the pathogenic mechanism is an influence. The scalp is the thickest pores and skin in the physique and absorbs a few of the power delivered to the pinnacle during impact.
Cheap 500 mg actoplus met otc
If renal substitute remedy turns into needed treatment diabetes gestational generic 500 mg actoplus met amex, then hemodialysis is the gold commonplace for remedy diabetes type 2 for dummies purchase 500mg actoplus met with amex. In patients which are hemodynamically unstable metabolic disease low blood sugar actoplus met 500 mg mastercard, steady renal alternative remedy is a viable choice. This mode of renal substitute remedy is well tolerated hemodynamically but is most likely not out there in all centers where cardiac surgery is performed. Sustained low-efficiency dialysis may be an alternative and may be carried out with routine hemodialysis gear. Initial trials have proven equivalence in medical outcomes when sustained lowefficiency dialysis is compared to steady renal replacement therapy. A lower in platelets inside 1 to 2 days after the preliminary postoperative enhance is more suggestive of immunologic etiology. Hematology Thormbocytopenia Platelets have an integral function in the expression of coronary artery disease and are equally essential within the postoperative cardiac surgical patient. The cornerstone within the management of ischemic coronary heart disease is the use of antiplatelet agents. These same agents can lead to excessive bleeding within the perioperative and postoperative part. This is extra a perform of the motion of platelets and not the quantity of platelets. Thrombocytopenia is outlined as a platelet count of a hundred and fifty,000 or much less platelets per milliliter and extreme thrombocytopenia as 50,000 or much less platelets per milliliter. The devastating and doubtlessly life-threatening side of this dysfunction pertains to the thrombotic issues owing to the induction of antiplatelet antibodies attributable to publicity to heparin. This reaction can happen in up to 10% of patients and causes platelet clumping or sequestration. This thrombocytopenia is gentle and transient with returned to regular platelet rely inside four days after stopping heparin. Heparin combines with platelet issue four and this interplay results in an immunoglobulin G antibody that activates platelets. The subsequent launch of prothrombotic particles from the platelets leads to an extreme thrombin formation, platelet aggregation, and thrombus formation. Because the antibody is so delicate there are false-positive outcomes and a serotonin release assay might have to be obtained for affirmation. However, argatroban can extend the prothrombin time and worldwide normalized ratio, which makes institution and monitoring of warfarin impact troublesome. The brief half-life of argatroban allows it to be discontinued for a few hours to decide the prothrombin time/ international normalized ratio when a affected person is taking warfarin so as to separate the person drug effects. Finally, platelet transfusion ought to be prevented unless the affected person is actively bleeding as further platelets may further gas the thrombotic impact. Anemia Blood loss anemia is by far the commonest purpose for transfusion on this inhabitants. The problem comes about as a result of multiple studies have shown that transfusion in cardiac surgery is related to increased morbidity and mortality. Optimization should happen before surgical procedure with iron administration and when acceptable, erythropoietin. Postoperatively these patients may need continued erythropoietin with iron administration, and judicious phlebotomy is advisable. The analysis was entertained by the findings of pain disproportionate to bodily findings, lactic acidosis, and leukocytosis. It is at that time that operative intervention could also be successful, earlier than bowel rupture and peritoneal contamination. When peritoneal signs are present on bodily examination, surgery is way much less successful. Pancreatitis Hyperamylasemia is fairly common in the early postoperative phase however clinical pancreatitis is uncommon and seen in only about 1% to 3% of cardiac surgical patients. True symptomatic pancreatitis is rare in this inhabitants however carries a high mortality due to its affiliation with a quantity of organ system failure. Treatment of pancreatitis begins and ends with bowel rest and nasogastric drainage. Antibiotics remain a source of controversy as indiscriminate dosing can lead to choice of more resistant organisms, whereas this exuberant inflammatory state can be tough to distinguish from sepsis. The widespread thread in the pathophysiologic mechanism is sympathetic vasoconstriction, with resultant hypoperfusion and hypoxia of the splanchnic mattress. Intestinal Ischemia Intestinal ischemia is a rare however extremely deadly complication of cardiac surgical procedure. The intraoperative monitoring with transesophageal echocardiogram may result in trauma to the esophagus. Aspirin, along with antiplatelet actions, might have a localized, topical effect on the gastric mucosa. Arterial venous malformations are unpredictable and could be corrected with interventional colonoscopy if they seem to be the source of recurrent blood loss. Diverticular disease and hemorrhoids may be a problem due to straining with bowel actions. Anesthesia, narcotic administration, psychological inhibition, and immobility contribute to the shortage of normal bowel habits. Stool softeners and fiber are used instantly postoperatively however over the following few days laxatives may be necessary to keep away from straining. The emphasis is avoidance of agents that may perpetuate or extended insult and injury, which can result in a delayed recovery. A nasogastric feeding tube may be a brief means for treatment administration and nutritional assist. Anorexia or nausea is incessantly seen in those emerging from anesthesia and usually resolves after 24 to 36 hours. Narcotic analgesia might delay the signs and sufferers respond to antiemetics or promotility agents. Patients require a more thorough workup after that initial time interval if symptoms persist. This may be associated to watery feces passing round an impaction because constipation is extra common instantly after surgical procedure. Stool softeners, laxatives, and promotility agents could also be missed as they might be a half of the postoperative order set. Magnesium oxide is a standard trigger for more and more frequent free bowel actions because low magnesium is aggressively corrected owing to the priority for arrhythmias. Patients receiving tube feeds may benefit from a much less hyperosmolar concentrated formulation or by administration of water with the feeds to dilute the osmolarity of these feeds. It is estimated that roughly 25% of patients will develop a transient hyperbilirubinemia but few progress to frank liver failure.
Buy actoplus met 500 mg free shipping
This may be accomplished with saline or sodium bicarbonate infusions and may be enhanced further by means of loop diuretics diabetes alert dogs in florida order 500mg actoplus met otc. Diuretic-induced quantity contraction must be averted because it will result in diabetes mellitus vascular complications purchase 500mg actoplus met with visa decreased distal nephron flow and decreased potassium excretion does diabetes type 1 shorten your life quality 500 mg actoplus met. It follows that the remedy of continual hyperkalemia is primarily directed towards stimulating renal potassium excretion whereas limiting potassium intake. For all adults with continual hyperkalemia, daily potassium consumption ought to be restricted to 60 mmol. All medication identified to impair both inner or exterior potassium stability should be eradicated if attainable. Finally, all patients with persistent hyperkalemia ought to be evaluated for occult urinary tract obstruction. In cases of mineralocorticoid unresponsiveness or when mineralocorticoid remedy is complicated by fluid overload, a thiazide or loop diuretic may be added to the regimen. This will restore normal volume status and enhance renal tubular potassium secretion in many mineralocorticoid-resistant sufferers. It is essential to avoid diuretic-induced quantity depletion, however, since this will exacerbate the renal potassium secretory defect. Patients who fail to reply to the previous measures may be given sodium bicarbonate, which will stimulate renal potassium secretion. The usual dose is 1 to 2 mmol bicarbonate/kg body weight per day in 3 or 4 divided doses. In patients with kidney perform discount of any degree, the infusion price must be halved (0. If the patient is still dangerously hypokalemic at this level, extra potassium may be given. Physiology of Water Homeostasis Normal plasma sodium concentration varies very little-even lower than the "regular" range of clinical laboratories (135�145 mmol/L). Tonicity or efficient osmolality describes the capacity of particles in resolution to effect water movement throughout a semi-permeable membrane like the cell membrane. The regular response to water ingestion (of sufficient magnitude to decrease the plasma osmolality even slightly) is the excretion of maximally dilute urine (urine osmolality <100 mOsm/kg). The underlying physiologic sequence is as follows: the plasma hypotonicity is sensed by the cells comprising the hypothalamic osmostat. This, in turn, creates a more water-impermeable conduit, stopping water reabsorption and permitting excretion of the dilute urine elaborated by the more proximal segments of the nephron. Notice that the minimal urine osmolality is about 50 mOsm/kg, and the maximum is about 1200 mOsm/kg. At that point, neurologically intact people with entry to water will drink until the plasma osmolality returns to regular. They are frequent problems in critically ill sufferers and are associated with elevated morbidity and mortality. Indeed, patients with persistent hyponatremia, even in the range of 115 to a hundred and twenty mmol/L, could additionally be completely asymptomatic. Most cells-especially brain cells-have adaptive mechanisms for mitigating tonicity-related volume changes. Thereafter solute and water are misplaced from cells, and cell quantity returns towards normal. After several days of sustained hypotonicity, cell quantity is restored to near regular. Between a hundred and twenty and 110 mmol/L, headache, lethargy, confusion, agitation, and obtundation may be seen. Isotonic hyponatremia (also known as factitious or pseudohyponatremia) is a laboratory artifact seen with analytic techniques that measure the mass of sodium per unit quantity of plasma sampled. Direct potentiometry (which uses an ion-selective electrode in undiluted plasma) avoids this problem. Hypotonic hyponatremia is brought on by an incapability of the kidney to excrete adequate electrolyte-free water to match water consumption. This could occur both as a outcome of the traditional diluting capacity of the kidney is overwhelmed by excessive water intake or as a end result of the diluting capacity of the kidney is impaired. These options usually could be distinguished by measuring the urine osmolality. It is a prodigious feat for a person consuming a traditional diet to overwhelm the traditional diluting capacity of the kidney. Estimates are that one can ingest (and excrete) about 20 L of water a day without affecting the plasma osmolality appreciably. The patient could also be ingesting a food plan so poor in protein and salt that he excretes little or no solute in the urine. In that state of affairs (called beer potomania for obvious causes,192 although the syndrome has been seen in different sufferers with very low day by day solute intake193), the low daily solute excretion limits the total quantity of water that may be eliminated even with a maximally dilute urine. This would possibly cut back the maximum water excretion to only three to four L/day, a quantity simply exceeded by an enthusiastic beer drinker. Hypotonic hyponatremia could also be related to normal, decreased, or increased extracellular quantity. Patients with pure water extra seem clinically euvolemic as a result of the excess water distributes throughout the whole physique water space; only one-third of complete body water is extracellular (and solely one-twelfth is intravascular). The solely proof of the slight intravascular quantity growth is low blood urea nitrogen and plasma uric acid concentration. Because the normal response to extracellular hypotonicity is the elaboration of maximally dilute urine (urine osmolality <100 mOsm/kg), the urine want only be inappropriately concentrated. They fall into five main classes: intracranial abnormalities, intrathoracic abnormalities, tumors, drugs, and idiopathic. The prognosis of reset osmostat syndrome has essential therapeutic implications, as mentioned later. Hyponatremia has just lately been acknowledged to happen with some frequency in endurance-sports athletes. The incidence of hyponatremia, with serum sodium ranges below a hundred thirty five mmol/L, is roughly 15% in marathon and triathlon athletes; 0. Excessive water intake is crucial factor in the improvement of hyponatremia for runners. The mechanism of hyponatremia on this setting is similar to that of different hypovolemic states. Particularly complicated in patients with cerebral salt losing is the finding of hypouricemia, which is thought to reflect impaired solute reabsorption within the proximal tubule. Thiazides have been associated with the event of acute severe, symptomatic hyponatremia, significantly in small, elderly girls, within the absence of overt indicators of volume depletion.
Purchase 500 mg actoplus met with visa
The loudness of the murmur diabetes drugs online actoplus met 500 mg sale, which correlates to some extent with severity metabolic disease zombie order actoplus met 500 mg without prescription, can be not specific because physique habitus and a wide selection of other factors have an effect on the acoustics transmitted across the chest diabetes diet hong kong buy actoplus met 500mg without a prescription. In this setting the murmur could also be fairly delicate, though typically nonetheless high-pitched because of the high velocity across a good constriction. A useful technique of differentiating aortic sclerosis from stenosis is that in the former the systolic ejection murmur heard over the proper sternum is typically mid-peaking and gentle to average in depth, and it features a well-preserved aortic second coronary heart sound. In contrast, if pulmonary hypertension is current, the P2 element may be exaggerated and may doubtlessly masks the diminished A2. A second component, described by Gallavardin as a musical element, is best heard at the left decrease sternal border. The latter confounds prognosis as a outcome of the murmur is Noninvasive Evaluation In contrast to the physical examination, echocardiographic methods have progressively improved over the past several many years and availability within the crucial care setting in industrialized nations is ubiquitous. The severity of calcification correlates with extent of obstruction by middle age, and usually Doppler sign velocity with peak and mean stress gradient and valve area by continuity equation present an correct total assessment. Several caveats need to be thought-about earlier than acceptance of noninvasive data within the critical care setting. Inadequate acoustic home windows in some patients and problem in positioning sufferers supported by respirators and with multiple lines in place do restrict echocardiographic imaging. C, However, a repeat continuous Doppler with care to keep away from mitral regurgitant circulate showed the true aortic velocity of two. Cardiac Catheterization Cardiac catheterization is indicated in sufferers in whom the noninvasive knowledge are equivocal (Box 30. Surgery with out coronary angiography is cheap for sufferers requiring emergency valve surgical procedure for acute valve regurgitation, disease of the aortic sinuses or ascending aorta, or infective endocarditis. It is important to distinguish between true severe aortic stenosis and pseudo-severe aortic stenosis. The differentiation could be made with dobutamine infusion (typical peak dose 20 �g/kg per minute). An exponential rise in gradient happens when move is elevated with valve areas within the severe stenosis range (<1 cm2). The curve demonstrates that change in gradient is proportional to the sq. of change in flow; thus doubling the move rate ends in a fourfold increase in gradient. Hydraulic formula for calculation of the world of the stenotic mitral valve, other cardiac valves, and central circulatory shunts. Because of the dependence on preload, a nice threshold exists between optimum filling pressures and pulmonary edema. Inotropic brokers are regularly required, and sufferers with insufficient contractile reserve could present limited improvement. Lipid-lowering therapy and changing enzyme inhibitors have been the subject of substantial investigation, though their position is within the continual setting quite than throughout important care. Both lipid-lowering and converting enzyme inhibitors have to be examined in bigger populations earlier in the midst of aortic valve disease. Therapy Medical Management Medical management is aimed solely at patient stabilization as a end result of pharmacologic intervention has never been proven to delay life and may obtain modest hemodynamic improvement at best. Stretching of the commissures is short-term, and any hemodynamic advantage of the latter resolves inside hours. Most valves have restenosed inside a few months, and the overall outcomes if no further intervention is performed are very poor; one sequence reported an 87% mortality price after a median period of less than 7 months. A successful 50% reduction in gradient occurs, however residual gradient stays at 50 mm Hg, nonetheless in the extreme category. The pulse strain has increased from 60 to ninety mm Hg, the height aortic systolic strain has elevated to one hundred forty mm Hg from a hundred mm Hg, and the aortic pressure upslope may be seen to have improved dramatically. Tissue valves are sewn to both balloon expandable or self-expanding stents, which are crimped onto a catheter and superior throughout the stenotic native valve. D, Mortality in the B cohort, showing substantial survival advantage among the 179 patients present process transcatheter aortic valve alternative over the 179 sufferers treated with medical therapy. In common, the danger of stroke appeared to be largely related to patient comorbid conditions that enhance stroke risk, rather than the kind of valve alternative. The stage of anticoagulation after surgery is restricted to prosthetic valve type and location. The former group consists of bicuspid and different aortic valve abnormalities, endocarditis, rheumatic aortic valve disease, the atherosclerotic course of described earlier, connective tissue problems, antiphospholipid syndrome (Libman-Sacks endocarditis), and toxicity from anorectic medicine. The abrupt rise in pressure is mirrored by parallel development of left atrial and pulmonary vascular hypertension, regularly resulting in pulmonary edema. The broad pulse pressure (150 mm Hg) difference between peak and minimal aortic strain (blue arrow) and close to diastasis of left ventricular and aortic pressure late in diastole (red arrow) are demonstrated. Early closure of the mitral valve might lead to a delicate first heart sound, and distortions of leaflet anatomy might result in lack of a distinct aortic second coronary heart sound. In some circumstances absence of a second coronary heart sound in a patient presenting with cardiogenic shock will be the most outstanding physical discovering. A wide pulse pressure outcomes primarily because of increased stroke volume, which augments systolic pressure108 and low aortic diastolic pressures because of volume runoff into the left ventricle. An additional consideration pertains to sufferers with aortic root dilatation (aortic root dimension >45 to 55 mm with the thresholds varying for sufferers with bicuspid valves or Marfan syndrome). It is essential to remember that these threshold values can be confounded by comorbid conditions that affect chamber dimension and performance, together with ischemic and different forms of cardiomyopathy, as well as multivalvular disease. Conduction disturbances remain an necessary characteristic, particularly coronary heart block within the setting of endocarditis, discussed subsequently. Cardiac catheterization in this setting normally includes aortic root angiography, though the latter requires a major dye load (typically 30 mL/s for as much as 2 seconds) to be diagnostically accurate. Tachycardia disproportionately decreases the diastolic filling interval, thereby reducing the period of regurgitation across the aortic valve. Oral vasodilators which have been described as having potential therapeutic benefit embrace a quantity of dihydropyridine calcium channel blockers (nifedipine and felodipine), in addition to hydralazine. The appropriateness of vasodilator therapy regardless of severity of disease is clearer in patients with systemic hypertension, in whom discount of afterload has dual benefits. The dose of drug ought to be enough to show at least some reduction in systolic pressure. In the crucial care setting, inotropes and vasodilators are appropriate if patients have congestive coronary heart failure, a low output state, or each. Special consideration ought to be given to sufferers with acute aortic valve endocarditis. Distortion or dysfunction of any of the weather and changes in function and geometry of the left ventricle and left atrium can all have a major impact on flow throughout the mitral valve. In addition, unlike different valvulopathies, the mitral valve is extremely dependent on the myocardial circulation. In distinction with the relatively passive nature of opening and closing of the aortic valve, mitral valve motion is an energetic process reflecting not only cyclical pressure variations but additionally tethering and dynamic interplay with the supporting apparatus. This mixture leads to each strain and quantity overload that appears to have an additive impact on severity of signs in addition to on outcomes. The incompetent mitral valve acts as a second pathway for blood ejection, which reduces afterload in a setting by which preload is elevated, thus potentiating ejection via the Frank-Starling mechanism.
Syndromes
- Unsteadiness
- Cough that produces mucus; it may be clear or yellow-green
- Umbilical stump bleeding
- Convulsions
- Extra fingers or toes (polydactyly)
- Urine protein
- What drugs, vitamins, herbs, and other supplements you are taking, even ones you bought without a prescription
- Blood pressure changes - can be extreme (autonomic hyperreflexia)
- Normal changes in the heart include deposits of the "aging pigment," lipofuscin. The heart muscle cells degenerate slightly. The valves inside the heart, which control the direction of blood flow, thicken and become stiffer. A heart murmur caused by valve stiffness is fairly common in the elderly.
- Dry the ears well after bathing or swimming.
Buy 500mg actoplus met overnight delivery
Iatrogenic pneumothoraces ensuing from thoracentesis improve the morbidity price diabetes type 1 hair loss discount actoplus met 500mg online, mortality price diabetes mellitus eye complications generic 500mg actoplus met with visa, and size of hospitalization diabetes risk factors order actoplus met 500 mg on-line. Previous stories indicated chest tube insertion could also be required in up to 50% of instances with a mean duration of placement of approximately four days. Statistically vital threat elements for creating thoracentesis included performing thoracentesis as a therapeutic procedure versus as a diagnostic procedure; the presence of cough, dyspnea, or chest ache in the course of the procedure; and witnessing the aspiration of air in the course of the procedure. Various mechanisms could clarify the pneumothoraces that happen after thoracentesis; the lung may be punctured at the time of needle entry or after the fluid has been withdrawn, or a small quantity of air may be drawn into the chest throughout aspiration or along the needle observe if excessive negative intrapleural strain develops. The first reported case of pneumothorax as a complication of passing a narrowbore feeding tube was in 1978. These factors permit undetected entry of the tube into the tracheobronchial tree, perforation of pulmonary tissue, and lodging in the pleural cavity. Normally, to affirm the proper placement of a feeding tube in the stomach, a small quantity of air is injected. This produces a attribute gurgle within the left higher quadrant of the abdomen, but a "pseudoconfirmatory gurgle" with a feeding tube within the chest has been reported. Findings related to pneumothorax included troublesome percutaneous dilational trache ostomy and the use of a fenestrated cannula. Special Situations Pneumothorax after partial decision of complete bronchial obstruc tion,146 as a complication of lobar collapse,147 and after therapeutic thoracentesis for malignant effusions148 has been described. Acute lobar collapse leads to a sudden improve in negative pleural stress surrounding the collapsed lobe. Although the parietal and visceral pleural surfaces stay intact, the fuel originating from the ambient tissues and blood is drawn into the pleural house, producing a pneumothorax referred to as pneumothorax ex vacuo. Recognition of this kind of pneumothorax is essential as a result of managing it requires relieving the bronchial obstruction somewhat than inserting a chest tube. The diagnosis of trapped lung requires documentation of chronicity and absence of pleural inflammation, pleural malignancy, or endobronchial lesion. The pathognomonic radiographic sign of a trapped lung is the pneumothorax ex vacuo, characterized as a small to moderatesized air collection after evacuation of effusion. Manifesta tions include dyspnea, chest ache, tachycardia, hypotension, cyanosis, distended neck veins, tracheal deviation, hyperresonance to percus sion, unilateral lower in breath sounds, and accompanying subcutaneous emphysema in roughly 25% of instances. If a pneumothorax results in severe hypoxemia or hemodynamic compromise, instant pleural decompression is required. This is normally accomplished by inserting a largebore needle into the second intercostal house in the midclavicular line of the affected hemithorax, adopted by tube thoracostomy. Tension Pneumothorax With a tension pneumothorax, the pleural pressure in the affected hemithorax exceeds atmospheric strain, specifically throughout expiration. This is often the result of a verify valve mechanism that facilitates the ingress of fuel into the pleural house during inspiration however blocks the escape of fuel from the pleural space throughout expiration. The results are the accumulation of gas leading to a buildup of stress inside the pleural area. The traditional indicators of a rigidity pneumothorax are deviation of the trachea away from the facet with the tension, an elevated percussion notice, and a hyperexpanded chest that moves little with respiration. Clinically unstable sufferers should undergo immediate needle decompression Sport-Related Pneumothorax Pneumothorax as a result of blunt trauma from contact sports is a recognized but underreported occasion. Several instances of pneumothorax or pneumomediastinum sustained throughout a contact sport have been described within the literature. Barotrauma Unrelated to Mechanical Ventilation Although the term barotrauma has historically been used to describe the event of extraalveolar air throughout mechanical air flow, in different instances it might be because of elevated intraalveolar stress, causing air to leak out of the alveoli. Pulmonary edema and hemorrhage occur when lung volume decreases under residual volume. As a diver ascends and transalveolar stress exceeds 20 to 80 mm Hg, overexpansion damage within the type of alveolar rupture can happen. Patients with a history of spontaneous pneumothorax, bullae, or cystic lung illness are at increased danger of pneumothorax and must be cautioned against diving. Note the mediastinal shift to the right, widened rib spacing, and posterior rib fractures on the left (white arrows). Decompression is carried out by advancing a normal 14 or 16gauge intravenous catheter into the pleural house at the junction of the midclavicular line and the second or third intercostal space. The needle is advanced until air could be aspirated right into a syringe linked to the needle. An immediate rush of air out of the chest signifies the presence of a pressure pneumothorax. The maneuver basically converts a rigidity pneumothorax into a simple pneumothorax. Electrocardiographic Features the presence of a pneumothorax could lead to distinct electrocar diographic adjustments, which may be mistaken for myocardial ischemia or infarction. Chest pain and dyspnea are the 2 major symptoms related to the development of pneumothorax. One collection evaluated 39 sufferers who presented with one of the two symptoms and 64% of them had both. Possible physical findings when a large pneumothorax is current embody decreased chest excursion on the affected side, diminished breath sounds, and hyperresonant percussion. Labored respiration accompanied by hemodynamic compromise (tachycardia or hypotension) suggests a potential pressure pneumothorax, which necessitates emergency decompression. As the stress continues to enhance, the diaphragm is flattened, the mediastinum is shifted to the other aspect, and ultimately cardiopulmonary collapse outcomes. Hypoxemia is frequent as a end result of collapsed and poorly ventilated parts of lung continue to obtain important perfusion. However, hypercapnia is unusual as a outcome of underlying lung function is comparatively normal and sufficient alveolar ventilation can be maintained by the contralateral lung. In certain conditions, the signs of pneumothorax could have an atypical presentation and subsequently require a excessive index of suspicion. During a transbronchial biopsy, a affected person could complain of pleuritic chest pain followed by dyspnea. A pneumothorax after a subclavian vein catheterization may current with progressive dyspnea and an alteration of important signs. In a mechanically ventilated patient, the initial presentation may embrace hypotension, newonset respira tory misery, unilateral lower in breath sounds, a lower in static and dynamic compliance, and worsening oxygenation. Patients can develop a persistent pleuropleuro channel after present process a median sternotomy, mediastinal surgery, or coronary heart or heartlung transplant surgical procedure. This situation has been dubbed "iatrogenic buffalo chest" as a outcome of the North American buffalo is one of few mammals which have speaking pleural areas. The primary characteristic of a pneumo thorax on a chest radiograph is a white visceral pleural line. A pneumothorax could also be recognized using an upright, supine, or lateral decubitus chest radiograph. Upright Chest Radiograph In an upright patient with a pneumothorax, most pleural gas accumulates in an apicolateral location.
Buy 500 mg actoplus met otc
Between the onset and end of the trial diabete et miel buy discount actoplus met 500 mg on line, the failure group developed will increase in Rinsp metabolic disease of erie purchase actoplus met 500 mg amex,L (P < zero diabetes mellitus in dogs client handout purchase actoplus met 500mg overnight delivery. Over the course of the trial, the failure group had larger values of Rinsp,L (P < zero. Pathophysiologic foundation of acute respiratory distress in sufferers who fail a trial of weaning from mechanical ventilation. In weaning-failure sufferers twitch Pdi values are beneath 10 cm H2O, whereas values of 35 to 39 cm H2O are observed in healthy subjects. Stimulation of the phrenic nerves and recording of the ensuing Pdi additionally provide probably the most direct measure of diaphragmatic fatigue. Cardiovascular Performance During a weaning trial, sufferers can experience substantial increases in proper and left ventricular afterload. At the completion of a weaning trial, the level of oxygen consumption is equivalent in weaning-success and weaning-failure sufferers. How the cardiovascular system meets the oxygen demand differs in the two groups of patients. In weaningsuccess sufferers, oxygen demand is met through an increase in oxygen supply, mediated by the anticipated enhance in cardiac output on discontinuation of positive-pressure air flow. At the beginning of the trial, the inspiratory tour in Pes was greater within the failure sufferers, and it increased additional by the top of the trial. To generate these plots, move and Pes tracings were divided into 25 equal time intervals over a single respiratory cycle for every of the 5 breaths for each patient within the 2 groups. For a given patient, the 5 breaths from the beginning of the trial have been then superimposed and aligned with respect to time, and the typical at each time point was calculated. The group mean tracings were then generated by ensemble averaging of the individual mean from every affected person. Instead, it results from speedy, shallow respiration, which causes a rise in dead-space ventilation. Pitfalls in Use of Weaning-Predictor Tests Physicians commonly view diagnostic testing in monolithic terms: a check is a test is a take a look at. In actuality, diagnostic testing has to fulfill two very different duties; one is screening, the other is affirmation. This occurs when a new examine population contains fewer (or more) sick patients than the population in which a diagnostic test was originally developed. This happens when the outcomes of a test beneath evaluation are used to choose sufferers for a reference-standard take a look at, corresponding to use of a weaning-predictor test to select patients for a reference-standard test (passing a weaning trial that results in extubation). The patients breathed spontaneously for an average of 44 minutes earlier than a physician terminated the trial. As the trial progressed, the tension-time index increased and the anticipated time to growth of task failure decreased. In different phrases, physicians interrupted the trial on the basis of clinical manifestations of respiratory misery before sufferers had adequate time to develop contractile fatigue. Rapid, shallow respiratory developed almost immediately after discontinuation of the ventilator. A good diagnostic check achieves a marked enhance (or decrease) in the posttest chance (over pretest probability). In reality, testreferral bias, a standard prevalence in studies of weaning tests, results in main adjustments in sensitivity and specificity. This was additionally the perspective of an Evidence-Based Medicine Task Force that undertook a metaanalysis of the research. A spontaneous breathing trial that entails 30 to a hundred and twenty minutes of monitored performance is the antithesis of a screening take a look at. Yet the EvidenceBased Medicine Task Force recommends that clinicians ought to start weaning with a spontaneous respiratory trial (a confirmatory test) and use the preliminary couple of minutes of the trial as a screening test. The observed positive predictive worth in a examine is plotted towards the pretest probability of weaning success (prevalence of profitable outcome). Initially 5 to 10 minutes in duration, T-tube trials are prolonged and repeated several times a day till the affected person can maintain spontaneous air flow for a quantity of hours. This approach has turn out to be unpopular as a result of it requires considerable time on the a half of intensive care staff. The noticed negative predictive value in a research is plotted in opposition to the pretest likelihood of weaning success (prevalence of profitable outcome). If the trial is unsuccessful, the patient is given a minimal of 24 hours of respiratory muscle relaxation with full ventilator support before one other trial is carried out. It is important to make a distinction between using a protocol in conducting a research examine and its use in everyday medical follow. When conducting analysis, this is precisely how a protocol have to be specified and followed. Extubation Decisions about weaning and choices about extubation are generally combined. Before removing the endotracheal tube, however, the clinician should additionally choose whether or not or not the affected person will be able to maintain a patent upper airway after extubation. It may be associated to the development of recent issues after extubation or to complications associated with reinsertion of a brand new tube. A extra likely clarification is that the necessity for reintubation displays larger severity of the underlying sickness. On elimination of the tube, the mucosal swelling produces a rise in upper airway resistance. Straus and associates forty six demonstrated experimentally that the respiratory work dissipated towards the supraglottic airway after extubation is almost identical to the work dissipated in opposition to an endotracheal tube earlier than extubation. Thus applying any stage of strain help causes physicians to underestimate the respiratory resistance a affected person will encounter after extubation. The addition of a small quantity of stress assist produces surprisingly large reductions in inspiratory work in ventilated patients: 5 cm H2O decreases inspiratory work by 31% to 38% and 10 cm H2O decreases work by 46% to 60%. Of the opposite three studies, two studies39,forty have been marred by main issues of internal validity. In abstract, solely half of one examine of six revealed legitimate assist for protocolized weaning, with the rest providing no proof of benefit. Physicians, nevertheless, are extremely conscious that respiratory frequency and tidal quantity are key variables in deciding whether or not a affected person will tolerate weaning and extubation. Because each step constitutes a diagnostic test, clinicians should be conscious of the scientific rules of diagnostic testing when decoding the information generated by each step. The crucial step is for the physician to contemplate the possibility that a patient just might be ready to tolerate weaning. Such diagnostic triggering is assisted through the use of a screening check, which is the rationale for measurement of weaning-predictor exams.

Buy 500 mg actoplus met visa
In this multicenter insulin or medication diabetes order 500 mg actoplus met with amex, randomized diabetes type 2 new medication buy actoplus met 500 mg with amex, placebo-controlled trial diabetes zits buy generic actoplus met 500 mg online, there was no distinction in the rate of development of septic shock between sufferers handled with a 50-mg bolus followed by a 200-mg steady infusion of hydrocortisone and these that received placebo. A high index of suspicion is necessary as a end result of the situation could be lethal if missed. The side effects of a brief course of high-dose corticosteroids in a critically sick affected person are minor in contrast with the potential consequence of cardiovascular collapse and death. Recommendations for the analysis and administration of corticosteroid insufficiency in critically ill adult patients: consensus statements from a global task force by the American College of Critical Care Medicine. Relative adrenal insufficiency in sufferers with septic shock: comparison of low-dose and traditional corticotropin checks. Adrenocortical function: an indicator of severity of illness and survival in chronically ill sufferers. Biphasic changes in hypothalamopituitary-adrenal operate in the course of the early restoration interval after main stomach surgery. Plasma corticotropin releasing factor and vasopressin responses to hypoglycemia in regular man. Plasma corticotropin releasing issue and vasopressin responses to exercise in regular man. Stress induced increase in vasopressin and corticotropin releasing issue expression in hypophysiotropic paraventricular neurons. Tumor necrosis factor alpha inhibits the hormonal response of the pituitary gland to hypothalamic releasing factors. Tumor necrosis factor as a potent inhibitor of adrenocorticotropin induced cortisol production and steroidogenic P450 enzyme gene expression in cultured human fetal adrenal cells. Adrenal autoantibodies bind to adrenal subcellular fractions enriched in cytochrome c reductase and 5-nucleotidase. Comparative results of prednisone and, cortisone in suppressing the response of the adrenal cortex to exogenous adrenocorticotropin. Hypothalamopituitary dysfunction following traumatic mind injury and aneurismal subarachnoid hemorrhage: a scientific evaluate. Interstitial cortisol obtained by microdialysis in mechanically ventilated septic sufferers: correlations with total and free serum cortisol. Variability of cortisol assays can confound the diagnosis of adrenal insufficiency in the critically sick inhabitants. Should we use etomidate as an induction agent for endotracheal intubation in patients with septic shock Diagnosis and remedy of major adrenal insufficiency: an Endocrine Society clinical practice guideline. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in sufferers with septic shock. Single induction dose of etomidate versus other induction brokers for endotracheal intubation in critically ill patients. The full or relative deficiency of glucocorticoids affects the quantity standing, vascular tone, and cardiac contractility immediately and indirectly. Patient with chronic obstructive pulmonary disease that requires pulse-dose prednisone a number of occasions a 12 months d. Patient with recurrent anaphylaxis requiring short-course steroids twice a 12 months Answer: c. What is the most applicable sequence of care for a hemodynamically unstable patient with suspect adrenal insufficiency Parenteral steroids, isotonic fluids, vasopressors, serum cortisol testing Answer: d. The administration of parenteral steroids and isotonic fluids should be carried out concomitantly. Which of the next medications has not been shown to trigger adrenal insufficiency However, patients receiving propofol maintain the response to the cosyntropin stimulation take a look at. Based on survey and administrative data obtained in Japan between 2004 and 2008 the annual incidence of thyroid storm was estimated at zero. Thyroid Physiology Thyroid Hormone Synthesis Thyroid tissue consists of spherical cavities called follicles, every lined with epithelial cells (follicular cells or thyrocytes) that encompass a cavity containing a colloidal suspension of a protein called thyroglobulin. Because T4 can be transformed in vivo into T3, and because T3 has substantially higher biological activity, T4 may be thought of a prohormone. Iodide egress at the apical membrane has been ascribed to an anion transporter referred to as pendrin. Iodide is transported from the cytoplasm to the follicle cavity by the anion transporter pendrin (P). Among the 2768 amino acid residues comprising each monomer of the dimeric protein thyroglobulin are 66 tyrosine moieties, 2 of that are depicted in the thyroglobulin section shown inside the follicular cell. The iodinated thyroglobulin is then taken again up by the follicular cell by way of pinocytosis and subjected to digestion by proteolytic enzymes (depicted by saw-toothed circular icons) after merger of the colloid droplet with intracellular lysosomes. The thyroid additionally produces a proportionately smaller amount of triiodothyronine in an analogous manner (not shown). The follicle thus serves as a response chamber for the creating thyroid hormones and likewise serves as a colloidal storage reservoir of hormone precursor. Each thyroglobulin molecule accommodates a quantity of T4 residues, but typically both one or no T3 residues. Via pinocytosis, follicular cells can then take in the modified thyroglobulin protein molecules, forming intracellular vesicles (colloid droplets) that fuse with intracellular lysosomes, thereby subjecting thyroglobulin to proteolytic enzymes that hydrolyze the protein into its constituent amino acids, releasing completed T3 and T4 molecules within the course of. Iodide inhibits each this intrafollicular cell breakdown of thyroglobulin and the next launch of thyroid hormones into the blood. Free T3 and free T4 are absorbed by most tissues all through the physique by the use of monocarboxylate transporters positioned on the cell membranes. After T3 enters peripheral cells it binds to intracellular thyroid hormone receptors, which act within the nucleus to promote or inhibit transcription of genes that broadly management basal metabolic fee, affect carbohydrate and lipid metabolism, regulate heat production, and influence a host of other systemic and very important organ processes, including body temperature, air flow, heart rate, cardiac output, and protein metabolism. Because D2 can take away just one iodine atom from the outer fragrant ring (specifically designated as the 5-carbon position), this enzyme can also be referred to as 5-deiodinase. D1 shares this 5-deiodination ability but can also take away one iodine atom from inside aromatic ring of T3 or T4. D1 is located on the plasma membrane of peripheral cells, whereas D2 (the main activating isoform) is intracellular and localized to the endoplasmic reticulum. D3 also deactivates T3 by removing an inside ring iodine atom to form three,3-diiodothyronine (3,3-T2). The deiodinases thus serve to regulate peripheral manufacturing of T3 from circulating T4 and also regulate intracellular T3 and T4 concentrations by controlling the initial steps of their catabolism.
Purchase actoplus met 500mg without a prescription
This phenomenon outcomes from ongoing cell metabolism in vitro with glucose and potassium uptake diabetes educator test generic actoplus met 500mg with mastercard. Pseudohypokalemia Hypokalemic Periodic Paralysis Therapeutic Hypothermia Pharmacologic Agents potassium adaptation in continual kidney disease diabetes mellitus merck purchase actoplus met 500 mg amex. Hyperkalemia in the setting of unexplained hypotension should immediately raise suspicion for adrenal insufficiency diabetes mellitus aafp buy actoplus met 500mg with mastercard. A common setting for isolated mineralocorticoid deficiency is the syndrome of hyporeninemic hypoaldosteronism. These medication are reported to be implicated in 10% to 38% of hyperkalemia in hospitalized sufferers. High- and low-dose heparin therapy decreases circulating aldosterone ranges by selectively inhibiting aldosterone biosynthesis. Two antibiotics, pentamidine128 and trimethoprim,129,one hundred thirty trigger hyperkalemia, often extreme, by blocking sodium reabsorption within the distal nephron. Chronic Hyperkalemia Renal Failure Chronic Hypokalemia Chronic hypokalemia is nearly all the time the results of altered external balance: inadequate potassium consumption, extreme potassium losses, or a mix of the two. Thus only huge gastric fluid losses would, alone, considerably deplete complete body potassium shops. The gastric fluid losses, however, stimulate renal potassium secretion in a quantity of methods. First, by generating a metabolic alkalosis and growing bicarbonate supply to the distal nephron, potassium secretion is stimulated. The metabolic alkalosis also leads to mobile proton loss and potassium uptake, which in renal epithelial cells, enhances potassium secretion. Thus on this state of affairs, urinary potassium focus is typically excessive while urinary chloride concentration is low owing to volume contraction. Those medication that act proximal to the potassium secretory site in the nephron promote a kaliuresis by rising supply of fluid distally and inflicting secondary aldosteronism. Thus hypokalemia frequently accompanies the utilization of the 2 commonest courses of diuretics: thiazides and loop diuretics. Mineralocorticoid excess may be primary137 (Conn syndrome) or secondary to diminished real or "effective" circulating quantity. All glucocorticoid medicine besides dexamethasone possess some mineralocorticoid exercise. Magnesium deficiency is associated with renal potassium losing and may lead to extreme potassium depletion (see later text). Because magnesium, like calcium, acts to stabilize excitable membranes, the deleterious results of hypokalemia on the myocardium are magnified by concurrent hypomagnesemia. Hypercalcemia causes a salt and water diuresis and is due to this fact commonly related to renal hypokalemia (see "Calcium"). Bartter and Gitelman syndromes are related to quantity contraction and regular blood pressure, and Liddle syndrome with hypertension. Clinical Manifestations of Hyperkalemia Hyperkalemia depolarizes the cell membrane, slows ventricular conduction, and reduces the period of the action potential. Normal electrocardiograms occur regardless of excessive hyperkalemia144 and the primary cardiac manifestation of hyperkalemia could additionally be ventricular fibrillation. Neuromuscular Effects Cardiac Effects Hyperkalemia may result in paresthesias and weak point progressing to a flaccid paralysis, which generally spares the diaphragm. Cardiac Effects Hypokalemia hyperpolarizes the cell membrane and prolongs the cardiac action potential. Hypokalemia could also be related to an increased incidence of arrhythmias and conduction defects. It is properly established that potassium depletion will increase the cardiac toxicity of digitalis glycosides. There is a rise in benign ventricular ectopy in hypokalemic sufferers without acute myocardial ischemia. In individuals hospitalized with acute myocardial infarction, nonetheless, a correlation between hypokalemia and ventricular tachycardia and fibrillation was observed. This normally includes the extremities however could progress to embrace the trunk and muscle tissue of air flow. As with hyperkalemia, cranial nerves typically are spared and sensory function usually remains intact. Conversely, in sufferers with hypokalemia and hypocalcemia, tetany could develop only after potassium replacement. In addition to the consequences of potassium depletion on the electrical properties of the neuromuscular system, profound hypokalemia may result in muscle harm and frank rhabdomyolysis, even in bedbound patients. Urine ought to be examined for heme pigments to exclude acute rhabdomyolysis or hemolysis. In the absence of that diagnosis, the affected person is prone to have either selective aldosterone deficiency and/or tubular unresponsiveness to aldosterone. Patients with hypokalemia upon presentation must be evaluated as though their hypokalemia were acute. Potassium excretion lower than 20 mmol/day suggests applicable renal potassium conservation and points to extrarenal Hypokalemia and potassium depletion are related to glucose intolerance,one hundred fifty five increased protein catabolism, polydipsia and polyuria,59 and metabolic alkalosis. In the presence of such signs, treatment for hyperkalemia should begin urgently (see "Treatment of Potassium Imbalance"). Excretion of higher than 20 mmol/day is proof of inadequate renal potassium conservation, indicating a renal reason for the hypokalemia. Renal potassium losses related to normal systemic blood pressure are mostly seen with the use of thiazide or loop diuretics and are accompanied by a metabolic alkalosis. Other causes of hypokalemia with metabolic alkalosis in a normotensive affected person include gastric fluid loss and Bartter and Gitelman syndromes. These are separable most often by historical past, but when not, the urinary chloride measurement will be helpful, being low with gastric fluid losses. Renal hypokalemia may accompany a renal tubular acidosis, during which case the plasma bicarbonate shall be low. Mineralocorticoid excess will be the trigger if the renal potassium loss is associated with systemic hypertension, and the reninaldosterone axis should be studied with basal and saline solution� suppressed blood hormone measurements. Acute Hyperkalemia In considering when hyperkalemia constitutes an emergency, two points must be kept in mind. Moreover, the extracellular quantity load imposed by hypertonic saline solution argues against its use. The putative advantages of a bolus injection of sodium bicarbonate within the emergency therapy of hyperkalemia pervaded the literature till lately. Ironically, this dogma was based mostly on research utilizing a prolonged (4�6 hours) infusion of bicarbonate. When given orally, the onset of motion is at least 2 hours and the maximum effect will not be seen for 6 hours or extra. Hemodialysis is the dialytic methodology of alternative for removing of potassium from the physique. However, renal potassium excretion may be enhanced even in patients with moderate renal failure by growing distal nephron move. Hyponatremia is seen in more than 20% of sufferers presenting with decompensated congestive coronary heart failure and greater than 30% of sufferers admitted to the hospital with problems of hepatic cirrhosis.
Order 500mg actoplus met with mastercard
Several terms have been used to describe these infections: necrotizing fasciitis; synergistic necrotizing cellulitis; progressive bacterial synergistic gangrene; anaerobic cellulitis; and diabetes test bangalore effective actoplus met 500mg, when muscle is concerned with clostridial an infection diabetes prevention drugs generic 500mg actoplus met with mastercard, clostridial myonecrosis (gas gangrene) diabetes test kit free purchase actoplus met 500mg mastercard. A number of options of some of the most necessary necrotizing pores and skin and soft tissue infections are proven in Table fifty one. Course Pain Gas formation Appearance Drainage Very rapid ++++ ++ Bullae, necrosis Serosanguineous Muscle ++++ Depth of involvement Skin, soft tissue Systemic toxicity � -, Absent; �, occasionally present; +, minimal; ++, delicate; +++, reasonable; ++++, marked or severe. Risk factors for these infections embody diabetes, old age, peripheral vascular illness, malignancy, alcoholism, renal failure, and immunosuppressive therapy. Diagnostic analysis must also embrace blood cultures, Gram staining of tissue exudates, and cardio and anaerobic cultures obtained at surgery or from a needle aspiration. Incision and exploration or biopsy may even be done at the bedside to obtain material for Gram stain, tradition, and histologic evaluation. Once a necrotizing delicate tissue an infection has been recognized, immediate therapy is essential. It occurs after trauma or quite lots of surgical procedures, perirectal abscess, decubitus ulcer, or perforation of the intestines. Patients at increased threat embrace those with diabetes mellitus, alcoholism, and injection drug use. The concerned space is initially erythematous and painful, however over several days pores and skin modifications embrace shade modifications, formation of bullae, and cutaneous gangrene. The involved space becomes anesthetic secondary to thrombosis of small blood vessels and destruction of superficial nerves. Anesthesia may develop earlier than the appearance of pores and skin necrosis and is a crucial clue to the presence of necrotizing fasciitis somewhat than easy cellulitis. Infection usually develops at a web site of trauma however may happen in the absence of an apparent portal of entry. Infection spreads broadly in deep fascial planes with relative sparing of the overlying skin and subsequently will not be acknowledged. This form of necrotizing fasciitis is current in roughly 50% of cases of streptococcal toxic shock syndrome. Bullae then rupture and evolve into an space coated by necrotic eschar, often resembling a third-degree burn. Streptococci can often be cultured from fluid of the early bullae and frequently from blood. Complications include metastatic abscess formation, and the mortality fee from this infection is high. Treatment requires surgical supply control with immediate surgical debridement and empiric broad-spectrum antibiotics. Initially the patient may be erroneously diagnosed with an acute abdomen until the genitalia are examined. Clostridial Myonecrosis (Gas Gangrene) Gas gangrene is a life-threatening an infection of skeletal muscle most incessantly caused by Clostridium spp. The position of hyperbaric oxygen remedy in the treatment of clostridial myonecrosis or in the remedy of necrotizing fasciitis remains controversial. In type I, no less than one anaerobic species is isolated together with a number of facultative anaerobes and members of the Enterobacteriaceae. Recent advances in genetic evaluation have led to the reclassification of some Vibrio spp. Identification of Vibrio organisms within the medical laboratory utilizing conventional methods may be troublesome. Serologic findings might provide supportive proof or may be useful in epidemiologic evaluation. Therapeutic choices embody third-generation cephalosporins, fluoroquinolones, and trimethoprim-sulfamethoxazole. Treatment for uncomplicated circumstances is 12 to 14 days; 30 days of remedy could additionally be needed for metastatic foci. There is a propensity to infect preexisting intravascular lesions such as atherosclerotic plaques and aneurysms. Sickle cell anemia and the presence of an orthopedic prosthesis are danger components for osteomyelitis. Secondary peritonitis most often arises from an enteric supply or pelvic focus and consists of peritonitis following an acute perforation of the gastrointestinal tract, intestinal necrosis, postoperative peritonitis that might be secondary to an anastomotic leak, and posttraumatic peritonitis following blunt or penetrating stomach trauma. Intestinal ischemia and frank necrotic bowel may be attributable to a selection of processes, together with malignancies, vascular insufficiency, volvulus, or intussusception. Localized lower abdominal peritonitis can even result from gynecologic infections such as salpingitis and endometritis. Tertiary peritonitis is described as occurring when scientific and systemic indicators of peritonitis persist or recur after treatment for secondary peritonitis. A distinct form of device-associated peritonitis is seen in sufferers undergoing peritoneal dialysis. Bacterial peritonitis is often attributable to flora of the massive intestine together with aerobes, with E. Treatment with corticosteroids may masks typical indicators and symptoms, delaying the diagnosis. Signs might embrace abdominal rigidity, distention, fever, and an total toxic look. A rigid abdomen may be seen in the early phases of an acute peritonitis, though it may be absent in a peritonitis that progresses more slowly, corresponding to that caused by tuberculosis, or when sterile bile, pancreatic fluid, or urine leaks into the peritoneal cavity. Aspiration of peritoneal fluid is an important part of the evaluation for peritonitis. Studies performed on peritoneal fluid ought to embody a cell depend with differential blood cell count, amylase, Gram stain and aerobic and anaerobic cultures, acid-fast smear and culture, and fungal smear and tradition. Serious Gastrointestinal and Intra-abdominal Infections Bacteremia Associated With Enteric Pathogens In widespread with pathogens that cause inflammatory diarrhea, the gram-negative organisms that trigger enteric fever syndrome are invasive. Enteric fever is normally caused by Salmonella enterica serotype typhi and infrequently by Salmonella paratyphi, Salmonella choleraesuis, Yersinia enterocolitica, Brucella spp. Physical findings embrace "rose spots," which are 2- to 4-mm discrete, irregular, blanching pink macules that are typically seen on the anterior chest; hepatosplenomegaly; and relative bradycardia. Multiorgan system dysfunction can occur as a consequence of metastatic infection or immune advanced deposition. Liver function tests and a serum amylase stage could define a source in the liver, gallbladder, or pancreas. A plain film of the stomach or a chest radiograph might reveal free air under the diaphragm within the case of a ruptured viscus. Antibiotic remedy to cover gram-negative bacillary organisms and anaerobes must be initiated. Risk factors for resistant organisms corresponding to latest hospitalization, comorbidities, previous antibiotic remedy, and colonization must be thought of. Options for empiric therapy embody mixtures corresponding to a third- or fourth-generation cephalosporin or a fluoroquinolone with metronidazole or monotherapy with a -lactam/-lactamase inhibitor combination, a carbapenem, or a glycylcycline corresponding to tigecycline. Gram-positive cocci could additionally be seen in up to 20% of cases and anaerobes in less than 5%. Some sufferers might have abdominal tenderness or rebound tenderness, however these findings are much less frequent than in other types of peritonitis.
References
- Tang NL, Fan HP, Chang KC, et al. Genetic association between a chemokine gene CXCL-10 (IP-10, interferon gamma inducible protein 10) and susceptibility to tuberculosis. Clin Chim Acta 2009; 406: 98-102.
- Donaldson K, Aitekne R, Tran L, et al. Carbon nanotubes: a review of their properties in relation to pulmonary toxicology and workplace safety. Toxicol Sci 2006;92:5-22.
- Nakagawa Y, Nagai T, Okawara H, et al. Cap polyposis (CP) which relapsed after remission by avoiding straining at defecation, and was cured by Helicobacter pylori eradication therapy. Intern Med. 2009;48(23):2009-2013.
- Nolan CM, Sandblom RE, Thummel KE, et al. Hepatotoxicity associated with acetaminophen usage in patients receiving multiple drug therapy for tuberculosis. Chest 1994; 105: 408-411.