

Forxiga
Denise M. Fitzpatrick, RNC, MSN, CNE
- Course Coordinator
- Abington Memorial Hospital, Dixon
- School of Nursing
- Willow Grove, Pennsylvania
Forxiga dosages: 10 mg, 5 mg
Forxiga packs: 14 pills, 28 pills, 42 pills, 56 pills, 70 pills, 84 pills, 98 pills

Buy 10mg forxiga free shipping
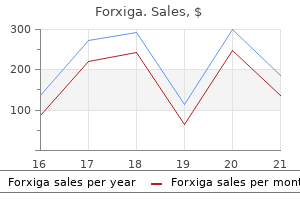
Furthermore diabetes mellitus education purchase forxiga 5 mg visa, fatty acids might impair calcium homeostasis and improve the manufacturing of free radicals vorbereitung diabetes test cheap forxiga 5mg mastercard, resulting in diabetes test strips wanted generic forxiga 10 mg online electrical instability and ventricular arrhythmias. Following electrical stimulation of the abdominal wall, a painful response (visual analogue scale eight out of 10) elicits a stress response with important improve in cortisol, catecholamines, and glucagon, and a decrease in insulin sensitivity and glucose uptake (31). Although these metabolic modifications happen after surgical procedure in all sufferers present process major surgery and experiencing ache, there are certain patient populations in whom the catabolic response is exaggerated. Functional Impairment Muscle fatigue is characterized by a decreased capability to carry out actions of daily dwelling along with an element of depression and muscle weakness (Table 6-2) (27). Although the mechanism for muscle weakness has not been elucidated, it appears to be a mix of impaired nutritional intake, the inflammatory-metabolic response, immobilization, and a subjective feeling of fatigue (28). A lower in handgrip power has been found to be associated to the magnitude of surgical stimulus, and can last as lengthy as three to four weeks. Type 2 diabetic sufferers experience the next mortality and morbidity in response to surgical treatment and have a more extended convalescence than those who are nondiabetic (33). Insulin resistance is associated with catabolic modifications in protein and glucose metabolism (34,35). Recently, proof was offered that the catabolic response to colorectal surgery is certainly increased in sufferers with sort 2 diabetes mellitus as mirrored by a 50% larger protein loss, glucose manufacturing, and glucose plasma concentration (40). Cancer Malnutrition and depletion of lean physique mass are attribute of patients with cancer. Quantitative evaluation of preoperative protein catabolism in surgical sufferers turns into relevant as a outcome of the frequency of utmost types of undernutrition seems to decline. Contrary to earlier research reporting incidences of up to 40% on hospital admission (44), more modern stories indicate that severe malnutrition occurs in only 6% to 20% of hospitalized sufferers (45). Less than 5% of patients present process surgery for colorectal cancer are malnourished. Anorexia and reduced consumption, quite than changes in energy expenditure, result in unfavorable vitality steadiness (46). Evidence suggests a hyperlink between the incidence of weight loss and alterations in complete body protein catabolism. Circulating levels of blood glucose in diabetic and nondiabetic patients with surgical and medical pathologies. These outcomes confirm earlier observations that, in most cancers cachexia, a maladaptation to the starved state happens, with a continued mobilization of protein and calorie reserves in the face of a decreased consumption (48). This period of fasting is long sufficient to substantially deplete hepatic glycogen stores, thereby rising the demand for amino acids for gluconeogenesis rather than tissue repair (60). Animal studies confirmed that coping with stress is far improved if the animals enter the trauma underneath fed quite than fasted conditions (61,62). The effect of adjusting the metabolic setting from an overnight fasted to a fed state earlier than surgical trauma on the development of the catabolic response has solely lately been tested in people. Overnight therapy with glucose infusions prevented the postoperative decrease in insulin sensitivity (63), inhibited urinary urea excretion (64), and decreased fatigue, as mirrored by improved voluntary muscle function (65). Clinical studies demonstrating higher end result with preoperative vitamin, significantly in malnourished sufferers (66,67), additional emphasize that the avoidance of fasting before surgery could make patients much less susceptible to postoperative issues that result in a decreased length of hospital keep. Stimulation of afferent sensory and sympathetic fibers by tissue trauma and activation of efferent hypothalamopituitary pathways has been thought-about to be one of many primary launch mechanisms (69). The effect of neuraxial blockade on the endocrine and metabolic response has been extensively investigated beforehand (68), and a consensus exists on the importance of the nature of the blockade and the adequacy of analgesia. High doses of local anesthetics provide an adequate somatic and autonomic blockade that forestalls stimulation of the hypothalamicpituitary-adrenal axis and is able to attenuating the cortisol and catecholamine response. However, this depends upon the sort and focus of native anesthetic (68), as well as the extent of the block. There is still an lively seek for the ideal native anesthetic agent able to provide an enough block of afferent and efferent nervous fibers with minimal side effects. Evidence shows that a symmetrical block extended from T4 to S5 dermatomes effectively suppresses the sympathetichypothalamic response, if initiated earlier than surgical procedure and continued for a reasonable time frame, which appears to be forty eight hours (70). Although injection of local anesthetics in the subarachnoid house supplies a dense block with significant attenuation of catabolic hormones and gluconeogenic metabolites (71), this method is time restricted. The epidural block, in distinction, may be maintained past surgical procedure and as these local anesthetics may be injected and an enough sensory block monitored. The first group consists of surgery under the umbilicus, during which native anesthetics have been injected into the epidural house to provide totally different ranges of sensory block and the endocrine response has been measured. Aging In animals, experiments have proven that the acute stress response turns into blunted with age (49). This relative adrenal insufficiency undoubtedly contributes to the elevated morbidity and mortality observed in older sufferers. In the previous, it was anticipated that aged sufferers, due to a decrease in skeletal lean tissue mass and a proportional improve in visceral lean tissue mass would need an increased stress response and plasma glucose to present glycemic gas to their viscera. Therefore, the prevailing knowledge factors to an attenuation of the acute stress response in the aged. Regarding protein metabolism, aging is related to sarcopenia (loss of skeletal muscles). Although incompletely understood, the etiology of sarcopenia is multifactorial: An elevated first-pass hepatic extraction of dietary amino acids occurs that decreases substrate availability for protein synthesis (55). Furthermore, the synthesis of myofibrillar, mitochondrial, and myosin heavy chain proteins declines with age (56). They undergo from extra cardiorespiratory complications, have much less postoperative energy, and are slower to recuperate. The principal mechanisms are afferent neural stimuli (arrows on right) as a result of noxious surgical/trauma stimuli and local tissue components released at the trauma site; both of these categories of stimuli could additionally be related to pain. Interleukin-1 is launched from circulating macrophages and forms a part of the "inflammatory soup" that sensitizes nociceptors. Central responses to afferent stimuli contain hypothalamus and other central nervous system areas mediating the efferent humoral and neural components of the endocrine-metabolic response. Factors that will explain the demonstrated lowered inhibition of the surgical stress response by epidural analgesia during major (upper) stomach procedures in comparison with procedures in the lower stomach and lower extremities. Existent data recommend that the main cause is an inadequate afferent somatic and sympathetic block, whereas unblocked parasympathetic afferents probably are of minor importance. With the block of sympathetic hyperactivity, epinephrine response is abolished and the efferent sympathetic neural pathways to the liver are inhibited. Insulin sensitivity is preserved by neural blockade by way of inhibition of the catabolic hormones, both of which are liable for inhibiting peripheral glucose clearance. Recent research utilizing normoglycemic hyperinsulinemic clamp and labeled tracers have proven the constructive impact of epidural anesthetics in reversing postoperative insulin resistance (78). The manufacturing of gluconeogenic substrates can be inhibited, and oxygen consumption is reduced.
Discount 5mg forxiga free shipping
When the dose of local anesthetic was increased additional diabetes mellitus etiology cheap forxiga 10 mg visa, the mean fatal doses of lidocaine (67) diabetes insipidus lab values bun forxiga 10 mg with visa, ropivacaine (67) diabetic diet vs atkins buy discount forxiga 5mg online, and l-bupivacaine (68) have been 829%, 108%, and 78% larger than bupivacaine (67), respectively, with the cause of demise varying with the native anesthetic (Table 5-6). Bupivacaine was associated with the sudden onset of ventricular tachycardiafibrillation, but without hypoxia or acidosis. Lidocaine overdose led to respiratory despair, bradycardia, and hypotension, but with out arrhythmias, and demise was attributed to "pump failure. Conscious Pregnant Sheep Model the excessive proportion of fatalities in pregnant girls struggling bupivacaine toxicity has stimulated a lot analysis into whether being pregnant is related to any increased sensitivity to native anesthetic toxicity, with in vitro studies of rabbit myocardium suggesting that progesterone enhances the arrhythmogenicity of bupivacaine (69). The mannequin described in the previous section has been used to evaluate the effects of equimolar concentrations of lbupivacaine, bupivacaine, and ropivacaine in pregnant sheep, with two strategies of injection getting used: bolus to mimic inadvertent intravascular injection, and fixed fee infusion to mimic cumulative toxicity. Nonpregnant and pregnant ewes were randomized to obtain lidocaine (70), bupivacaine (71), ropivacaine (71,72), or l-bupivacaine at a relentless price of 0. In pregnant sheep, the dose threshold for convulsions was decrease than in nonpregnant animals, however no difference existed for the onset of cardiac arrhythmias. There had been no vital variations between pregnant and nonpregnant ewes in plasma drug concentrations, except in pregnant animals at the time of circulatory collapse (73). The rank order for toxicity was defined according to convulsive dose and plasma focus and was discovered to be within the sequence bupivacaine >l-bupivacaine >ropivacaine. Furthermore, there was no significant distinction between the three medication in uterine blood circulate or fetal plasma and tissue concentrations. The nature of the large-animal experiments used has various in accordance with the character of the scientific query being requested. A catheter was inserted into the left anterior descending coronary artery in anesthetized pigs and growing doses of drug had been injected. Early research consistently demonstrated a toxicity ratio of >15:1 for bupivacaine and lidocaine, 2. A comparable direct intracoronary injection examine was performed in sheep (76) utilizing incremental equimolar doses. Although two-thirds of the sheep died of ventricular fibrillation, no differences have been detected between medicine, in contrast to the studies within the pig model. Human Volunteer Studies Despite animal studies implying that each ropivacaine and lbupivacaine have a decrease degree of toxicity than bupivacaine, the ideal examine would show related effects in man. They then obtained, on separate days, 10 mg/min of bupivacaine, ropivacaine, or l-bupivacaine in crossover, randomized, double-blind studies. The first two research both showed that a bigger dose of ropivacaine (124 mg [77] and one hundred fifteen mg [78]) was tolerated higher than that of bupivacaine (99 mg [77] and 103 mg [78]). Both medicine impaired left ventricular systolic and diastolic perform in contrast with placebo, however the effect was greater with bupivacaine. Side results have been comparable apart from an increased incidence of muscle twitching in the volunteers given bupivacaine. The topics receiving bupivacaine had higher decreases in stroke index, acceleration index, and ejection fraction as measured by thoracic bioimpedance. The signs that occurred completely in the course of the ropivacaine infusion had been chest ache, circumoral paresthesia, ache, style perversion, and vasodilatation, whereas solely a feeling of detachment and hyperventilation occurred completely with l-bupivacaine. Levobupivacaine had less excitatory traits, judged in phrases of their magnitude and the extent of the brain involved, and the volunteers suffered more antagonistic occasions, such as tinnitus and dizziness, with bupivacaine. Large-animal and human volunteer studies have demonstrated that each l-bupivacaine and ropivacaine show a lowered propensity towards Ca arrhythmias, require larger doses for a lethal impact in animal fashions, and have much less effect on cardiac mechanical perform in human volunteers. Treatment As indicated earlier, prevention is healthier than a remedy, thus adequate patient analysis and preparatory steps are essential. Prior data of the differential prognosis of local anesthetic reactions can be vital. In the event of a systemic toxic response to any native anesthetic occurring on account of inadvertent intravascular injection or some other cause, full life assist measures should be instigated instantly. In common terms, administration should follow established guidelines corresponding to those of the American Heart Association (82) or U. A full-blown poisonous response, even with a drug corresponding to lidocaine, is life-threatening and requires skilled management if the affected person is to recover unharmed. Few will have to cope with multiple or two such occasions in a profession, so adherence to standard resuscitation protocols is necessary because the coaching given for different settings should imply that the routines are nicely ingrained (see Tables 5-7 to 5-9). May range with vasopressor used Rapidly reversible with elevation of legs Allergy Immediate Delayed High spinal or epidural block Concurrent medical episode. Medical historical past essential Sympathetic block above T4 adds cardioaccelerator nerve blockade to the vasodilation seen with blockade below T4; whole spinal block might have rapid onset. Local anesthetic toxicity may end in convulsions; nevertheless, with speedy and appropriate remedy, these ought to by no means be fatal in themselves. Some clinicians even designated a drug that had not been available for a quantity of years as their most popular, first-line agent for use in the event of native anesthetic�induced ventricular arrhythmias. The upkeep of full oxygenation will be an ongoing requirement needing fixed attention. If the onset of the reaction has not, perforce, resulted within the cessation of native anesthetic administration, then the clinician should be sure that this is the case. Interestingly, this enhanced toxicity is most likely not associated to greater myocardial uptake of drug as a end result of rabbit research have proven a decrease within the uptake of bupivacaine within the presence of acidosis (87). Thus, the extreme cardiovascular effects of the stronger medication such as bupivacaine may be due, in part no much less than, to an interplay with extreme acid�base changes. Hypercarbia, acidosis, and hypoxia, as can occur in some sufferers due to the metabolic consequences of vigorous muscle activity throughout seizures, could additionally be lowered by sufficient lung air flow with oxygen, however they may not be overcome. This is the rationale for taking a extra active approach to the management of convulsions. There is probably more than a modicum of truth in this, and it is very important check that the lungs are being ventilated adequately with 100% oxygen. Almost any drug with an anticon- Acidosis and Hypoxia It is inconceivable to overstress the importance of avoiding hypoxia and acidosis. The essential level is to observe the low doses advocated: these drugs are far more potent as anticonvulsants than as anesthetics, and use of anesthetic doses will add to the cardiovascular melancholy brought on by native anesthetic toxicity. Because of issues concerning the cardiovascular effects of sedative medicine, some advocate using this short-acting neuromuscular blocking drug in a dose of about 50 mg. Sparse evidence exists, despite firmly held opinions, as to the most effective technique of controlling convulsions. Each technique has its optimistic and negative features, and the clinician is suggested to suppose the matter through before the clinical want arises, so that treatment is prompt and applicable on the time. The nature of the cardiovascular collapse was completely different in the two species: electromechanical dissociation and asystole occurred within the canine, whereas ventricular fibrillation and asystole have been more likely in sheep. Furthermore, the initial dose of bupivacaine used to trigger cardiovascular collapse was sevenfold higher in canine (24.
Diseases
- Diffuse leiomyomatosis with Alport syndrome
- Myotonia atrophica
- Neonatal diabetes mellitus, transient (TNDM)
- Vertical talus
- Groll Hirschowitz syndrome
- Cold agglutination syndrome
- Buruli ulcer
- Mental retardation macrocephaly coarse facies hypotonia
- Oto-Palatal-digital syndrome
Buy forxiga 10mg with mastercard
Practice Guidelines for sedation and analgesia by non-Anesthesiologists: An updated report by the American Society of Anesthesiologists task force on sedation and analgesia by non-anesthesiologists metabolic disease that causes joint pain order 10mg forxiga mastercard. Responses to atropine diabetic diet drinks discount 5mg forxiga with amex, glycopyrrolate blood sugar is 300 order 10 mg forxiga mastercard, and Riopan of gastric fluid pH and volume in adult patients. The results of basic versus epidural anesthesia for outpatient extracorporeal shock wave lithotripsy. Single-injection paravertebral block compared to basic anesthesia in breast surgical procedure. Ropivacaine epidural anesthesia and analgesia versus general anesthesia and intravenous patient-controlled analgesia with morphine within the perioperative management of hip alternative. Postoperative complaints after spinal thiopentone-isoflurane anaesthesia in sufferers undergoing orthopaedic surgical procedure: Spinal versus general anaesthesia. Does multimodal analgesia with acetaminophen, nonsteroidal antiinflammatory drugs, or selective cyclooxygenase-2 inhibitors and patient-controlled analgesia morphine provide advantages over morphine alone Gabapentin and postoperative ache: Systematic evaluate of randomized controlled trials. Axillary plexus block using a peripheral nerve stimulator: Single or a quantity of injections. Brachial plexus block with the nerve stimulator: Motor response traits at three sites. Efficacy of a nerve stimulator in regional analgesia; experience in a resident coaching program. The use of the nerve stimulator with commonplace unsheathed needles in nerve blockade. Comparison of insulated and uninsulated needles for locating peripheral nerves with a peripheral nerve stimulator. Electrical characteristics of peripheral nerve stimulators: Implications for nerve localization. The electrophysiological impact of dextrose 5% in water on single-shot peripheral nerve stimulation. A technique to facilitate regional anaesthesia by detection of mixed nerve motion potentials. Percutaneous electrode steering and subcutaneous stimulating electrode steerage: Modifications of the original method. Stimulating popliteal catheters for postoperative analgesia after hallux valgus restore. Using stimulating catheters for continuous sciatic nerve block shortens onset time of surgical block and minimizes postoperative consumption of pain medicine after hallux valgus repair as compared with standard nonstimulating catheters. Does femoral nerve catheter placement with stimulating catheters improve effective placement Use of a stimulating catheter for total knee alternative surgical procedure: Preliminary results. Continuous femoral nerve analgesia after unilateral total knee arthroplasty: Stimulating versus nonstimulating catheters. Verifying correct placement of an epidural catheter tip using electrical stimulation. A prospective comparative research of two oblique strategies for confirming the localization of an epidural catheter for postoperative analgesia. Thoracic and lumbar epidural analgesia through the caudal approach using electrical stimulation steering in pediatric sufferers: A review of 289 sufferers. Cervical epidural analgesia via a thoracic method utilizing nerve stimulation guidance in an adult affected person present process elbow surgical procedure. Thoracic epidural catheter placement in infants through the caudal strategy beneath electrocardiographic steering: Simplification of the unique method. Ultrasound guidance speeds execution and improves the quality of supraclavicular block. Practice Guidelines for sedation and analgesia by non-anesthesiologists: An updated report by the American Society of Anesthesiologists task pressure on sedation and analgesia by non-anesthesiologists. Sedative infusions during native and regional anesthesia: A comparison of midazolam and propofol. A comparison of propofol with a propofol-ketamine mixture for sedation throughout spinal anesthesia. Comparison of responses to transmitter candidates at an Nmethylaspartate receptor mediated synapse, in slices of rat cerebral cortex. Concomitant administration of morphine and an N-methyl-D-aspartate receptor antagonist profoundly reduces inflammatory evoked spinal c-Fos expression. The benefits of intraoperative small-dose ketamine on postoperative pain after anterior cruciate ligament repair. Preemptive analgesia by intravenous low-dose ketamine and epidural morphine in gastrectomy: A randomized double-blind research. Intraoperative ketamine in combination with epidural analgesia: Postoperative analgesia after renal surgery. A comparability of dexmedetomidine versus typical remedy for sedation and hemodynamic management during carotid endarterectomy performed under regional anesthesia. Comparison of intravenous sedativeanalgesic techniques for outpatient immersion lithotripsy. Remifentanil or propofol for sedation throughout carotid endarterectomy beneath cervical plexus block. Remifentanil versus remifentanil/ midazolam for ambulatory surgical procedure throughout monitored anaesthesia care. Remifentanil, propofol or both for conscious sedation throughout eye surgical procedure under regional anaesthesia. Speed of restoration and side-effect profile of sevoflurane sedation in contrast with midazolam. Beyond this, anatomic understanding is required to avoid problems as a result of needle injury or incorrectly positioned injection, to understand the physiologic occasions resulting from neural blockade, and to develop new methods for anesthesia and pain remedy. This is in part as a end result of the particular interests of anesthesiologists in such issues because the organization of tissue planes and the permeability of assorted limitations that regulate distribution of fluids, interests shared by few other physicians and scientists. An further problem is the issue of observing the contents of the spinal canal, which are enclosed by sturdy bones and ligaments. Removal of these buildings disrupts the pure arrangement of the delicate tissues within the canal. This article anatomically tours the neuraxis, generally from outer to inside buildings, and includes new observations wherever potential. Errors are comparable within the sitting and mendacity positions, are higher with overweight topics, and are higher utilizing the vertebra prominens as a reference point compared to the Tuffier line (10,11). The numerical designations of the vertebra might differ between individuals because of anomalous patterns of vertebral segmentation, that are predominantly found in the lumbosacral spine (12). This parallels the phylogenetic stability of mammalian cervical and thoracic segmentation and the marked variability in the variety of lumbar vertebrae, even amongst primates (13). The last lumbar or first sacral vertebrae is often indeterminate in configuration, with fusion of L5 to S1 in 6.
Forxiga 5mg with mastercard
Thoracic epidural anesthesia increases diaphragmatic shortening after thoracotomy in the awake lamb control diabetes during pregnancy order 5mg forxiga otc. Lung perform under excessive thoracic segmental epidural anesthesia with ropivacaine or bupivacaine in sufferers with extreme persistent obstructive pulmonary illness present process breast surgical procedure diabetes symptoms missed period generic forxiga 10 mg with mastercard. Morphological indications for considerable diffuse reabsorption of cerebrospinal fluid in spinal meninges particularly in the areas of meningeal funnels blood sugar calculator buy 5 mg forxiga otc. The unfold of options injected into the epidural area: A research using epidurograms in patients with the lumbosciatic syndrome. Epidural area as a Starling resistor and elevation of circulate resistance in a diseased epidural space. Continuous positive airway stress respiration increases the unfold of sensory blockade after low-thoracic epidural injection of lidocaine. Epidural block for abdominal surgical procedure: Aspects of scientific pharmacology of etidocaine. The effect of subarachnoid lidocaine and combined subarachnoid lidocaine and epidural bupivacaine on electrical sensory thresholds. Effects of etidocaine administered epidurally on modifications in somatosensory evoked potentials after dermatomal stimulation. Effect of thoracic epidural bupivacaine on somatosensory evoked potentials after dermatomal stimulation. Effect of epidural bupivacaine on somatosensory evoked potentials after dermatomal stimulation. Effects of epidural bupivacaine or mepivacaine on somatosensory evoked potentials and skin resistance responses. Intraoperative loss of somatosensory evoked potentials predicts lack of spinal wire function. Quality of spinal extradural anaesthesia: the affect of spinal nerve root diameter. Segmental spread and predictability of epidural analgesia in youth and excessive age. Lumbar epidural anaesthetic with bupivacaine in old patients: Effect of velocity and direction of injection. The impact of age on the systemic absorption and systemic disposition of bupivacaine after epidural administration. The results of age on the neural blockade and hemodynamic changes following epidural anesthesia with ropivacaine. Perioperative myocardial ischaemia in patients present process surgery for fractured hip randomized to incremental spinal, single-dose spinal or general anaesthesia. Aging reduces the efficacy of the simulated epidural take a look at dose in anesthetized adults. Spread of analgesic options within the epidural house and their site of action: A statistical examine. Systemic toxicity and resuscitation in bupivacaine-, levobupivacaine-, or ropivacaine-infused rats. Myocardial and cerebral drug concentrations and the mechanisms of dying after intravenous doses of lignocaine, bupivacaine, and ropivacaine within the sheep. Comparative ventricular electrophysiologic effect of racemic bupivacaine, levobupivacaine and ropivacaine on the isolated rabbit coronary heart. Cardiovascular and central nervous system results of intravenous levobupivacaine and bupivacaine in sheep. Comparison of a chloroprocaine-bupivacaine combination with chloroprocaine and bupivacaine used individually for obstetric epidural analgesia. Role of epinephrine in regional block anesthesia with etidocaine: A double-blind examine. Effects of including adrenaline to etidocaine and lignocaine in extradural anaesthesia. Epidural epinephrine and clonidine: Segmental analgesia and results on totally different ache modalities. The effect of extradural ketamine on onset time and sensory block in extradural anesthesia with bupivacaine. Small-dose S(+)-ketamine reduces postoperative pain when utilized with ropivacaine in epidural anesthesia for total knee arthroplasty. Interactions between noradrenergic and cholinergic mechanisms concerned in spinal nociceptive processing. Study of three completely different doses of epidural neostigmine coadministered with lidocaine for postoperative analgesia. The position of plastic tubing in steady block strategies: An x-ray examine of 552 sufferers. An analysis of the radiological visualization of the catheters positioned in the epidural area. Continuous epidural analgesia, an uncommon case of dural perforation throughout catheterisation of the epidural house. The accuracy of using thiopental or test strips to detect dural puncture during continuous epidural analgesia. Cardiac resuscitation after incremental overdosage with lidocaine, bupivacaine, levobupivacaine, and ropivacaine in anesthetized canines. Resuscitation from bupivacaine-induced asystole in rats: Comparison of different cardioactive medication. Successful resuscitation of a affected person with ropivacaine-induced asystole after axillary plexus block. Levobupivacaine-induced seizures and cardiovascular collapse treated with Intralipid. Total spinal anesthesia late in the middle of obstetric bupivacaine epidural block. Accidental intravenous injection of bupivacaine: A complication of obstetrical epidural anaesthesia. Hazards of subdural and epidural anesthesia during anticoagulant therapy: A case report and evaluate. A comparability of the hydrochloride and carbonated salts of lignocaine for caudal analgesia in outpatients. Plasma willpower of lidocaine and bupivacaine after caudal anesthesia in children. Caudal anesthesia with lidocaine or bupivacaine: Plasma native anesthetic concentration and extent of sensory unfold in young and old sufferers. Plasma lidocaine concentrations after caudal, lumbar epidural, axillary block, and intravenous regional anesthesia. Comparison of anesthetic options utilized in lumbar and caudal peridural anesthesia. Clinical evaluation of etidocaine in steady caudal analgesia for pelvic floor repair and postoperative pain reduction. Blood concentrations of lidocaine, mepivacaine and bupivacaine during caudal analgesia in children. Age, peak, and pace of injection as elements determining caudal anesthetic stage, and incidence of extreme hypertension.
5mg forxiga with visa
Pain following thoracotomy can be intense type 2 diabetes mellitus leaflet cheap 10mg forxiga fast delivery, which may produce pulmonary problems following surgery (148) injectable diabetes medications weight loss generic 10mg forxiga amex. Many elements are involved within the occurrence of pulmonary dysfunction following thoracotomy managing diabetes 9 code buy generic forxiga 5 mg on-line. Postoperative changes in pulmonary operate result from lung resection, atelectasis, and/or quantity loss as a outcome of pneumothorax and also inspiratory muscle dysfunction. In addition, lung transplant recipients present process thoracotomy have a lower incidence of adequate ache reduction than patients undergoing thoracotomy for different indications (149). These medical observations emphasize that the condition of the affected person might play a major function (along with type of incision) relating to adequacy of postoperative pain management (149). Clearly, when compared to normal thoracotomy incisions, sufferers receiving minithoracotomy incisions expertise less postoperative ache and consume much less supplemental analgesics in the course of the quick postoperative period. Importantly, up to half of all patients undergoing thoracotomy incision will develop continual pain associated to the surgical website. Evidence exists that signifies enough postoperative ache management following thoracotomy might help forestall the development of persistent postoperative thoracotomy pain. Therefore, an effective postoperative analgesic plan have to be developed for these patients. In contrast to median sternotomy incisions and minithoracotomy incisions, there seems to be some clinical proof indicating that use of regional anesthetic strategies might lower postoperative complications following thoracotomy incisions. However, though ample proof exists suggesting that thoracic epidural analgesia offers superior postoperative analgesia, not all scientific research have proven that such techniques really enhance postoperative pulmonary perform and scale back postoperative pulmonary issues (Chapter 23). Clinical Outcomes All clinical stories involving utilization of intrathecal and thoracic epidural anesthesia and analgesia strategies for cardiac surgical procedure involve small numbers of patients and few (if any) are well designed (Tables 22-2 and 22-3). Only a handful of scientific research involving intrathecal analgesia are prospective, randomized, blinded, and placebo-controlled (Table 22-2). Furthermore, not one of the present clinical studies involving intrathecal and thoracic epidural anesthesia and analgesia techniques for cardiac surgery use scientific end result as a major end-point. Thus, clear deficiencies within the literature prohibit definitive analysis of the risk-benefit ratio of intrathecal and thoracic epidural anesthesia and analgesia methods as applied to patients present process cardiac surgery. Fifteen trials enrolling 1,178 patients were included for thoracic epidural anesthesia evaluation and 17 trials enrolling 668 patients were included for intrathecal analysis. These authors also notice that the risk of spinal hematoma (addressed later in this chapter) due to central neuraxial analgesia in sufferers present process full anticoagulation for cardiopulmonary bypass stays unsure. Ongoing controversy continues over correct choice of anesthetic approach and affect on consequence because vascular procedures usually lend themselves to all kinds of native, regional, common, or combined regional/general anesthetic techniques. Patients having vascular surgery are a novel group, with a high incidence of coexisting illness related to superior age, cigarette smoking, diabetes, and hypertension (among others). Coronary artery disease is easily the leading reason for perioperative mortality following vascular surgery, and long-term survival following these procedures is considerably restricted by a excessive incidence of morbid cardiac events. Given the systemic nature of atherosclerotic disease, very few patients who current for vascular surgical procedure have normal coronary arteries, and greater than half of the patients have superior or severe coronary artery illness (153). Needless to say, these patients often solely have borderline perform in essential organ techniques (heart, kidneys, lungs, etc. Furthermore, assessing perioperative risk in these sick individuals earlier than vascular surgery is a difficult and controversial task. Most operative procedures on the thoracic and/or belly aorta and its major branches require massive incisions and intensive dissection, clamping and unclamping of the aorta and its major branches, varying duration of organ ischemia, vital fluid shifts and temperature fluctuations, thus stimulating activation of the neuroendocrine stress response (most importantly during the instant postoperative period). The pathophysiology of aortic cross-clamping and unclamping is complex and is dependent upon many elements, including the extent of the cross-clamp, extent of coronary artery illness and myocardial dysfunction, diploma of aortic collateralization, blood volume and distribution, activation of the sympathetic nervous system, and the anesthetic agents/techniques utilized. Of greatest concern to the anesthesiologist managing these patients is adjustments in blood stress, systemic vascular resistance, cardiac output, and myocardial function with cross-clamp application and removal. Inadequate analgesia (coupled with an uninhibited stress response) through the postoperative period following vascular surgery (like cardiac surgery) may result in many adverse hemodynamic (tachycardia, hypertension, vasoconstriction), metabolic (increased catabolism), immunologic (impaired immune response), and hemostatic (platelet activation) alterations. In sufferers undergoing vascular surgery, perioperative myocardial ischemia is mostly observed during the instant postoperative interval and appears to be related to end result. Furthermore, postoperative myocardial ischemia may be aggravated by cardiac sympathetic nerve activation, which disrupts the steadiness between coronary blood flow and myocardial oxygen demand (27). Thus, in the course of the instant postoperative interval after vascular surgery, enough analgesia (coupled with stress response attenuation) might probably decrease morbidity and improve health-related quality of life (27,28). Because these procedures might typically progress to extra invasive arterial reconstruction, a regional or common anesthetic initiated earlier than the process begins might keep away from an unplanned and undesirable conversion to common anesthesia. In some sufferers, a selected anesthetic method (regional or general) may be preferable to others. Because sufferers undergoing vascular surgery usually have a surgical incision on the decrease half of the physique, the overwhelming majority of neural blockade methods in these patients involve intrathecal and/or epidural methods. Likewise, further potential advantages of using intrathecal and/or epidural methods in patients undergoing vascular surgical procedure embody stress response attenuation and thoracic cardiac sympathectomy. However, as with cardiac surgery, whether such enhanced postoperative analgesia, stress response attenuation, and thoracic cardiac sympathectomy through intrathecal and/or epidural methods actually affects morbidity and mortality in sufferers present process vascular surgery is controversial. Thoracoabdominal Aortic Reconstruction Perhaps no surgical procedure is extra challenging for the anesthesiologist than thoracoabdominal aortic reconstruction. Management points embrace lung separation, extracorporeal circulatory support, hypothermia, spinal twine safety, renal protection, hemodynamic instability, large blood losses, and coagulopathy, among others. Even in facilities the place numerous such surgeries are performed, morbidity and mortality remains high. Although the surgical incision is quite giant and painful (thoracic and belly cavities entered), most clinicians are hesitant to make the most of epidural strategies as a outcome of these sufferers are at elevated danger for epidural hematoma formation due to systemic heparinization (required for extracorporeal circulatory support), coagulopathy from hypothermia, and big transfusion. Heller and Chaney describe such a case in a affected person who underwent uneventful thoracoabdominal aortic aneurysm restore (154). On the primary postoperative day, the patient had full motor power and function of both decrease extremities and was ambulating without problem. At this time, ache was well-controlled with thoracic epidural infusion of bupivacaine 1. Seven hours after catheter removing, the patient was unable to transfer either decrease extremity in opposition to gravity. Ten hours after catheter removal, the affected person was unable to move both decrease extremity. Emergency magnetic resonance imaging revealed no signs of extradural mass or epidural hematoma, but demonstrated spinal twine infarction in the anterior spinal artery distribution. By the fifth postoperative day, sensory level to pin-prick had stabilized at T10, and the affected person had no motor function in his legs. The authors note that postoperative management of an epidural (lumbar or thoracic) catheter in a patient after thoracoabdominal aortic surgical procedure is definitely challenging and considerably controversial. However, in this distinctive affected person population, concern at all times exists regarding neurologic deficit associated to the surgical procedure itself. One might argue that, in this patient, the thoracic epidural infusion should have been immediately discontinued when the neurologic deficit was first noted and that magnetic resonance imaging ought to have been carried out earlier. Perhaps with earlier detection of spinal twine ischemia, prognosis in this affected person would have been altered. However, a study involving aortic occlusion in rats signifies that spinal administration of large doses of morphine after transient aortic occlusion may be related to a possible threat of paraparesis and the corresponding growth of neurologic dysfunction (156). These authors warning in opposition to using large doses of intrathecal morphine for postoperative analgesia in patients present process thoracoabdominal aortic aneurysm restore.
Syndromes
- Continue to wet the bed more than twice a month after age 5 or 6
- Knee joint pain when walking
- Antisocial personality disorder
- Head injury or nasal or sinus surgery
- Autoimmune hepatitis
- CT scan of the chest
Order forxiga 10mg overnight delivery
Vertebral level of termination of the spinal wire with report of a case of sacral cord diabetic food list buy discount forxiga 10 mg line. Biomechanical aspects of the subarachnoid area and cervical twine in healthy individuals examined with kinematic magnetic resonance imaging diabetic vodka buy forxiga 10mg free shipping. Medullary cone motion in subjects with a normal spinal wire and in patients with a tethered wire diabetes type 1 low cheap forxiga 10 mg with mastercard. Determination of the segmental sensory and motor innervation of the lumbosacral spinal nerves. The nerve provide of the vertebral column and its associated structures within the monkey. The nature and distribution of the innervation of human supraspinal and interspinal ligaments. Spinal projections of cat main fibers innervating lumbar facet joints and multifidus muscle. Lumbar disc lesion with particular reference to the histological significance of nerve endings of the lumbar discs. Immunohistochemical demonstration of nociceptors within the ligamentous constructions of the lumbar backbone. Substance P: Localization, concentration and launch in cerebral arteries, choroid plexus and dura mater. Immunohistochemical localization of substance P in the lumbosacral spinal pia mater and ventral roots of the cat. Localization of substance P and neurofilament immunoreactive fibers in the lumbar facet joint capsule and supraspinous ligament of the rabbit. Morphological basis for again pain: the demonstration of nerve fibers and neuropeptides in the lumbar facet joint capsule but not in ligamentum flavum. Discharge properties of mechanosensitive afferents supplying the retroperitoneal space. Characterization of spinal somatosensory neurons having receptive fields in lumbar tissues of cats. A quantitative examine of the central projection patterns of unmyelinated ventral root afferents within the cat. The spinal nerve root "innervation", and a model new concept of the clinicopathological interrelations in back pain and sciatica. Observations on the cause and mechanism of symptom-production in sciatica and low-back ache. The tissue origin of low back pain and sciatica: A report of ache response to tissue stimulation during operations on the lumbar spine using local anesthesia. Identification of distinct topographical distribution of lumbar sympathetic and sensory neurons projecting to finish organs with totally different capabilities within the cat. Sympathetic activation of cat spinal neurons aware of noxious stimulation of deep tissues in the low again. Electrical stimulation of the upper thoracic portion of the sympathetic chain in man. Pain responses on stimulation of the lumbar sympathetic chain beneath local anesthesia. On the nerve supply of the connective tissue of some peripheral nervous system elements. Three-dimensional evaluation of the vascular system in the rat spinal wire with scanning electron microscopy of vascular corrosion casts. Arterial vascularization of the spinal twine: Recent studies of the anastomotic substitution pathways. Preoperative spinal artery localization and its relationship to postoperative neurologic problems. Diffusion from the cerebrospinal fluid as a nutritional pathway for spinal nerve roots. The vertebral and azygos venous methods, and some variations in systemic venous return. The position of the vertebral venous system in the metastasis of most cancers to the spinal column. A technique of angiography of the azygos vein and the anterior inside venous plexus of the backbone. Comparison of intraosseous vertebral venography and Pantopaque myelography within the diagnosis of surgical situations of the lumbar spine and nerve roots. The significance of venous return impairment in ischemic radiculopathy and myelopathy. Distribution in spinal fluid, blood, and lymph of epidurally injected morphine and inulin in canine. The natural history of lumbar intervertebral disc extrusions handled nonoperatively. In the late nineteenth century, soon after the invention of the native anesthetic properties of cocaine, spinal anesthesia was launched into scientific practice. In the primary experiments and scientific use, the native anesthetic used was cocaine (Table 10-1) (1). Therefore, using spinal anesthesia was limited to a few fanatics until safer local anesthetics-procaine (2) and later tetracaine (3)-caused a widespread interest in its use. The growth of recent common anesthesia utilizing muscle relaxants and an endotracheal tube, together with the fear of neurologic problems, decreased the interest in spinal anesthesia in Nineteen Forties and Nineteen Fifties (6). As operations turned extra radical, their duration and extensiveness had been typically incompatible with spinal anesthesia. Dedicated fanatics, nevertheless, continued to use the strategy and imagine in its safety (7), and, about forty years ago, spinal anesthesia started to regain its place in anesthesia care. Since the 1980s, fashionable disposable needles and particularly the utilization of bupivacaine has tremendously elevated the interest in spinal anesthesia in plenty of nations (8,9). The proven reality that basic anesthesia additionally has its dangers and issues has made spinal anesthesia a priceless choice for surgical procedure of the lower abdomen and extremities. It is used in brief ambulatory procedures as a restricted saddle block or as unilateral anesthesia to present a fast, restricted, short-lasting, and reliable anesthesia with good-quality postoperative ache relief (10). The spinal anesthesia approach and dose, and the properties of the local anesthetic can be tailored to obtain optimum spread and duration of the anesthesia for the planned surgery. Specifically, spinal anesthesia is suitable in patients who select to stay aware or whose medical condition re- quires consciousness through the surgery, however who nonetheless need high-quality anesthesia. Patients with respiratory issues or tough airways may not need an endotracheal tube if spinal anaesthesia is employed. The threat of vomiting and aspiration is diminished (but not eliminated) during spinal anesthesia. Cholecystectomies and gastrectomies have successfully been performed under spinal anesthesia.
Discount forxiga 5mg overnight delivery
Propofol in combination with ketamine was initially used to try and diabetes 88 diet generic forxiga 5 mg free shipping reduce the hemodynamic effects sometimes seen with propofol infusion alone (80) diabetes insipidus zentrum proven forxiga 10mg. Later research appeared at the analgesic effect of propofol�ketamine infusion and demonstrated that the mix was related to a lowered requirement for "rescue" opioid doses oral diabetes medications for dogs order forxiga 5 mg amex, as in comparability with propofol alone, in sufferers present process breast biopsy procedures. This research advised that ketamine was a useful adjuvant to propofol sedation at an optimum propofol�ketamine dose ratio of 10:1 (81). It is our widespread medical follow to add 20 mg of ketamine to 20 mL of propofol (10 mg/mL) to produce a last focus of approximately 9 mg/mL propofol to 0. Intraoperative low-dose ketamine has additionally been demonstrated to considerably cut back postoperative opioid requirements (86� 88). Therefore, along with its preoperative and intraoperative benefits as a potent sedative and analgesic, intraoperative infusion of low-dose ketamine (0. The 2 -adrenergic receptor agonist clonidine, has been used as an anesthetic premedication, in addition to for perioperative sedation and intraoperative and postoperative analgesia. In regional anesthesia, clonidine is extra widely used as an additive to native anesthetics to delay and intensify the analgesic results of neural blockade and as an analgesic/anesthetic adjuvant for neuraxial blockade (89). The use of low-dose opioids alone to supplement regional anesthesia is of limited value. The mixture of an opioid analgesic and a benzodiazepine for sedation has been shown to cut back the necessities of both agents. For the nonanesthesiologist, the apply tips for sedation and analgesia as outlined by the American Society of Anesthesiologists are glorious fundamental ideas that every one ought to follow (77). The most common methodology of administering sedative and analgesic medication intraoperatively is intravenously. With development of more refined levels of technology, the single or combined uses of bolus, continuous drip, continuous infusion, and even patient-controlled administration are actually out there. The choice of strategies should be tailored to the circumstances of patient and process. For comparatively shorter procedures or for sufferers who request that very minimal sedation be administered intraoperatively, small doses of sedative drugs titrated in intermittent doses to obtain the desired impact may be most applicable. However, although the technique of intermittent dosing throughout the perioperative interval is possible, intraoperative administration of ongoing sedation in a secure surgical procedure can be simply accomplished utilizing any of quite so much of continuous infusion gadgets. A number of nonopioid medicine have been commonly used for intraoperative sedation for patients undergoing surgical procedures with regional anesthesia, together with barbiturates (methohexital, pentobarbital) and benzodiazepines (diazepam, midazolam). Midazolam, propofol (alone or in combination with ketamine), and dexmedetomidine are at present essentially the most generally used intraoperative sedative agents for patients with neural blockade. Midazolam, being probably the most generally used benzodiazepine for preoperative sedation and anxiolysis, is commonly used to produce intraoperative sedation as well. Effective dosing regimens for midazolam may be accomplished by both preliminary dosing of 1 to 2 mg, followed by subsequent intermittent doses of 0. In 1991, sedative infusions of midazolam had been compared to propofol throughout native and regional anesthesia. This early study demonstrated that, though the general high quality of sedation was similar in the two groups, using propofol was related to less postoperative sedation, drowsiness, and confusion, Chapter 8: Perioperative Management of Patients and Equipment Selection for Neural Blockade 177 lithotripsy in contrast with a purely epidural method (92). Caution and cautious monitoring are essential when combining opioid and benzodiazepine sedation for long procedures and/or in poor-risk patients. In a study of volunteers receiving fentanyl 2 g/kg, 50% developed hypoxemia as outlined by oxygen saturation (Sao2) of lower than 90% (93). The use of supplemental oxygen and sufficient monitoring of respiratory perform and hemoglobin oxygen saturation are important for all regional anesthesia techniques during which sedation and analgesia, alone or in combination, are used. The implementation of continuous infusion methods for intraoperative supplementation has led to the use of very potent, short-acting agents. In the opioid class of medication, remifentanil, a fentanyl derivative, has attracted interest. It is rapidly metabolized by tissue esterases, with a short, context-sensitive half-time of 3. Its transient period of action avoids the issue of postoperative respiratory depression but also offers no postoperative analgesia. The combination of midazolam with remifentanil potentiates the sedative and respiratory depressant effects of remifentanil (96). For patients requiring extra analgesia in addition to sedation for painful procedures, corresponding to retrobulbar block, the use of remifentanil (0. Three major reasons exist for combining inhalation strategies with a regional anesthetic approach. First, there are operative positions and procedures in regards to the head, neck, thorax, and higher abdomen that require endotracheal tube protection of the airway in opposition to obstruction or aspiration. Although patients in crucial care models tolerate indwelling endotracheal tubes with little or no sedation, most surgical patients need to be anesthetized if the endotracheal tube is to be tolerated during surgical manipulation. Second, procedures of very lengthy duration can be performed with regional anesthesia utilizing steady catheter techniques or long-acting native anesthetics corresponding to bupivacaine or ropivacaine. However, the cumulative doses of the parenteral sedatives and opioids can turn into very high over several hours of administration, leading to a prolonged postoperative restoration time. In these instances, as quickly as vital basal sedation is achieved with sedatives and opioids, it might be fascinating to change to low concentrations of inhaled agents. In some cases, the limitation of the regional anesthetic could additionally be anticipated, as in using thoracic epidural anesthesia for thoracotomy or upper stomach surgical procedure, where using a basic anesthetic in combination with the epidural anesthetic is the deliberate method. Anesthesiologists must always do not neglect that the objective is to provide the patient with the easiest anesthetic possible throughout the surgical procedure. For patients who dislike or resist the claustrophobic feeling of head straps and face masks, a nasal airway related to the circle breathing circuit of an anesthetic machine may be a passable various. The use of inhaled agents for supplemental sedation is quite common in dental practice. Nitrous oxide was historically the most well-liked of the supplemental inhalation brokers due to its important analgesic properties and its low efficiency, which give a wide margin of security. Recommended concentrations of nitrous oxide for "inhalation sedation" are 25% to 50%. An early research (98) involved 394 sufferers who obtained 1,005 outpatient dental treatments with the same old local anesthetic techniques plus a set focus of 25% nitrous oxide by way of a nasal mask. Ninety-nine percent of these patients acquired adequate analgesia without loss of consciousness. More essential, the change in anxiousness stage on subsequent treatments declined from the preliminary 86% who had been "very anxious" to lower than 10% on the fourth visit. Generally, these outcomes apply to the proper administration of most regional anesthetic procedures. Low concentrations of potent unstable anesthetics may also be used to present intraoperative sedation and analgesia. Patients respiratory isoflurane had been more relaxed, had marginally more speedy recovery and, in spite of a slightly disagreeable odor, would prefer isoflurane once more (100). Sevoflurane is enticing as an inhalation agent for sedation in sufferers with regional anesthesia because of its characteristics of nonpungency, fast onset, and fast elimination. However, sedation with sevoflurane was associated with a excessive incidence of intraoperative excitement, leading to conversion to common anesthesia (101).
Forxiga 5mg low cost
The whole onerous palate is equipped by the maxillary nerve by way of the sphenopalatine ganglion blood glucose 3 month test buy generic forxiga 10 mg on line. The recurrent laryngeal nerve additionally provides motor function to all of the intrinsic muscle tissue of the larynx (except the cricothyroid muscle) diabetes type 1 essay buy generic forxiga 5mg, and bilateral motor block produces loss of phonation and loss of capability to shut the glottis diabetes medications and side effects order forxiga 5 mg with visa. Palatine Nerve the palatine nerves are distributed to the roof of the mouth, soft palate, tonsil, and lining membrane of the nasal cavity. Most of their branches are derived from the sphenopalatine branches of the maxillary nerve. The anterior palatine nerve descends through the pterygopalatine canal and emerges within the hard palate via the greater palatine foramen. The center palatine nerve emerges by way of one of many minor palatine foramen and offers the sensory provide to the uvula, tonsils, and the taste bud. The posterior palatine nerve descends via the pterygopalatine canal and emerges by way of a special opening behind the higher palatine foramen. The center and posterior palatine branches be part of the tonsillar branch of the glossopharyngeal to form a plexus (cirrus tonsillaris) around the tonsils (7). Cervical Plexus the cervical plexus contributes to the provision of both the deep and the superficial constructions of the neck. The first cervical nerve, C1, is a motor nerve to the muscles of the suboccipital triangle and has no sensory distribution to skin. The pores and skin of the neck is supplied in a sequential dermatomal pattern (like the trunk) by the cutaneous branches of C2�C4 by both anterior and posterior main rami. The cervical plexus is formed by the ventral rami of the upper four cervical nerves. Their dorsal and ventral roots mix to kind spinal nerves as they exit via the intervertebral foramen. The cervical plexus lies behind the clavicular head of the sternocleidomastoid, giving out both the superficial and deep branches. The superficial cervical plexus wraps around the belly of the clavicular head of the sternocleidomastoid to kind four branches: (a) the lesser occipital, (b) the great auricular, (c) the transverse cervical, and (d) the supraclavicular nerves. It arises from the second and third cervical nerve roots, winds around the posterior border of the sternocleidomastoid and, after perforating the deep fascia, ascends behind the clavicular head of the sternocleidomastoid beneath the platysma to the parotid gland, the place it divides into an anterior and posterior branch. The anterior branch (ramus anterior; facial branch) is distributed to the pores and skin of the face over the parotid gland and communicates in the substance of the gland with the facial nerve. The posterior branch communicates with the smaller lesser occipital, the auricular department of the vagus, and the posterior auricular department of the facial nerve (7). In the area of the scalp, the nerves of supply have lengthy superficial upward programs. Mandibular Division (V3) of the Trigeminal Nerve the mandibular nerve emerges from the cranial cavity by way of the ground of the middle cranial fossa, by way of the foramen ovale, to enter the infratemporal fossa. This fossa is a rectangular compartment bounded anteriorly by the posterior wall of the maxilla and posteriorly by the styloid equipment and carotid sheath. The lateral wall is the ramus of the mandible, and the medial wall consists anteriorly of the lateral pterygoid plate of the sphenoid bone and posteriorly by the constrictor muscles of the pharynx. In the infratemporal fossa, the mandibular nerve divides into its terminal branches. Glossopharyngeal Nerve the glossopharyngeal nerve provides the posterior third of the tongue and the oropharynx from its junction with the nasopharynx on the degree of the exhausting palate. It provides the pharyngeal surfaces of the soft palate and the epiglottis, and the pharyngeal wall, as far down as the pharyngoesophageal junction at the degree of the cricoid cartilage (C6). With the advent of endotracheal intubation and extra subtle strategies for common anesthesia, its enchantment as a main surgical anesthetic declined. It has merit as a diagnostic block, a everlasting neurolytic block, and as a method Vagus Nerve the vagus nerve provides sensation to the larynx. The undersurface of the epiglottis and the laryngeal inlet all the method down to the vocal folds are supplied by the inner laryngeal branch of the vagus. This nerve reaches the larynx by piercing the thyrohyoid membrane, which joins the thyroid to the hyoid cartilages. Any of those constructions might be broken by the introduction of the needle through the foramen ovale. Technique A An 8- to 10-cm, 22-gauge needle is required for Gasserian ganglion block. In edentulous patients, this landmark may not permit a adequate angle of approach to enter the foramen ovale, and due to this fact a degree of insertion extra caudad is required. Such an approach usually causes the needle to impinge on the roof of the infratemporal fossa. The needle is then adjusted till it slips via the foramen ovale; normally, just previous to this, a mandibular nerve paresthesia is obtained within the lower jaw or lip. This maneuver is optimally (but not necessarily) performed beneath radiographic management, so that the needle and its path via the foramen ovale can be visualized (5). Initially, there might be a third-division mandibular paresthesia, however this could occur whereas the needle remains to be within the infratemporal fossa. A: Note that the needle is inserted within the cheek about 1 cm posterior to the angle of the mouth, as shown, and directed towards the pupil in the anterior view and the midpoint of the zygoma within the lateral view. The needle is then directed barely posteriorly (2) to get hold of a mandibular nerve (V3) paresthesia. C: the needle can then be superior via the foramen ovale into the middle cranial fossa, where it will be adjoining to the Gasserian ganglion, as proven. The Gasserian ganglion is reached with a needle by traversing the infratemporal fossa and entering the middle cranial fossa by means of the foramen ovale. Medially, the Gasserian ganglion is bounded by the cavernous venous sinus, which con- Confirmation: Caution: Complication: 10 Chapter 17: Somatic Blockade of the Head and Neck 411 Indications Supraorbital and supratrochlear nerve analgesia is an easy block that can produce glorious analgesia of the brow and scalp again from eyebrows to the vertex (6). These strategies could be utilized for surgery performed on the scalp, restore to lacerations, elimination of cysts, frontal craniotomies, midline dermoid excisions, frontal ventriculoperitoneal shunts, Omaya reservoir placement in neonates (2), and nevus excisions on the anterior portion of the scalp (6) (Table 17-3). Technique (Supraorbital Block) the supraorbital foramen is palpated on the roof of the orbital rim, roughly on the level of the pupil in most sufferers. A subcutaneous wheal of native anesthetic answer is injected with the needle directed parallel to the eyebrow at the web site of the needle insertion in a subcutaneous plane. Firm strain ought to be utilized to the world after the needle is withdrawn, stopping the formation of a hematoma. Clinical Application of Gasserian Ganglion Blockade in Pain States Local anesthetics injected into the ganglion can produce profound analgesia in sure pain states, such as tic douloureux (but only for short periods), and neurolytic blocks with alcohol had been used in the past by some therapists for this condition (5,12,13). The pain reduction is obtained on the price of hemifacial and corneal analgesia, with saliva typically dribbling out of the ipsilateral, numb aspect of the mouth. Such blocks, for longterm ache reduction, are hardly ever performed by ache specialists right now (Chapters forty two and 45).
Buy forxiga 10 mg fast delivery
This can be used for offering pain relief for posterior craniotomies as nicely for pain secondary to occipital neuralgia (33) diabetes mellitus in pregnancy cheap 10 mg forxiga overnight delivery. It is also a helpful block in each prognosis and remedy of occipital "pressure" headaches (Table 17-10) diabetes zentrum wandsbek forxiga 5 mg cheap. Superficial Cervical Plexus Block the cutaneous distribution of the cervical plexus is to the skin of the anterolateral neck by means of the anterior major rami of C2�C4 metabolic disease basal ganglia forxiga 10mg with mastercard. All 4 nerves can be blocked by infiltration on the midpoint of the posterior border of the sternomastoid. Indications Blockade of the superficial cervical plexus can present sensory analgesia for the postauricular space of the scalp (lesser occipital), the exterior pinna (30), and the posterior auricular area in addition to the temporoparietal area of the scalp (greater auricular), the anterior portion of the neck (transverse cervical) (31), and provide to the supraclavicular space (supraclavicular branch). The higher auricular nerve block has been successfully used for pain relief following tympanomastoid surgical procedure (4) and otoplasty (30). A 27-gauge needle is placed subsequent to the artery and within the subcutaneous aircraft whereas fanning laterally. After careful aspiration to rule out intravascular placement, 2 to three mL of native anesthetic answer is injected. Note the greater and lesser occipital nerve branches crossing the superior nuchal line approximately midway between the higher occipital protuberance and the mastoid course of. Superficial infiltration along this line will produce analgesia of the posterior scalp. The larger occipital nerve can be located by figuring out the pulsations of the posterior occipital artery, which crosses the nuchal line in firm with the nerve. This block is used together with blocks of the supraorbital, supratrochlear, auriculotemporal, and lesser occipital nerves to render the scalp anesthetized for surgery (2). Deep Cervical Plexus Block Indications this block is usually helpful for such procedures as thyroidectomy and tracheostomy under native anesthesia (although rarely, see later discussion), and can be used successfully for unilateral carotid endarterectomy or for unilateral elimination of cervical lymph nodes. Three needles are historically used, being inserted on the levels of C2, C3, and C4. The sites of insertion are situated by reference to a line that joins the tip of the mastoid course of with the Chassaignac tubercle of C6, which is readily palpated at the degree of the cricoid cartilage. This line lies over the "gutters" in the superior floor of the transverse processes, upon which the cervical nerve roots pass laterally. The C4 nerve root is located on the junction of the vertical line and a line horizontally drawn to the lower border of the mandible, with the pinnacle in a impartial place. The C3 and C2 nerve roots can be positioned by dividing the distance between the mastoid and horizontal line into thirds (see proper higher panel). Individual cervical nerve roots could additionally be blocked by injecting small volumes of local anesthetics, as shown within the higher proper. Single-injection block of cervical plexus can be obtained by a method similar to interscalene brachial plexus block, since the cervical nerve roots are contained in a continuous space between the scalene muscle tissue. A single needle is inserted on the vertical line at the C4 stage and directed medially and slightly caudad to contact the "gutter" of the transverse process (lower panel). Note that caudad path is important to avoid penetration of an intervertebral foramen, with attainable injection into epidural house or dural sleeve (and thus direct entry to cerebrospinal fluid). Note additionally the proximity of the vertebral artery passing by way of the foramina transversaria of the transverse processes. A horizontal line via the lower border of the ramus of the mandible intersects this line at C4; 5-cm, 22-gauge needles are directed medially and caudad. The cause for the caudad path is to keep away from getting into the intervertebral foramen and producing a peridural or spinal block. The end-point is the bony landmark of the transverse process, and paresthesias are obtained. Injection of 3 to four mL of 1% lidocaine or the equivalent on each nerve is usually sufficient for anesthesia. The paravertebral house communicates freely within the cervical region, and hence the anesthetic solution spreads easily to adjacent levels. Deep cervical plexus block subsequently can quite often be obtained with injections at just one level, with a bigger quantity of 6 to eight mL. Deep cervical plexus block is a frequent adverse effect following a single-needle interscalene approach for brachial plexus block. If digital pressure is maintained distally over the interscalene groove and the patient positioned in a horizontal (or even head-down posture), cervical plexus block may be predictably produced utilizing the identical needle insertion technique as for the interscalene brachial plexus block (Table 17-11). C2 transverse course of is one finger breadth under the mastoid process on this line, and C3 and C4 are related distances caudad. Needles are inserted medially and caudad till they attain the transverse process and paresthesias are obtained. Intravascular injection, brachial plexus blockade Complications: Complications A significant complication of the block is as a result of of the proximity of the vertebral artery, as a outcome of unintentional direct intra-arterial injection could produce profound and very rapid poisonous side effects of convulsions, unconsciousness, and blindness; therefore, aspiration exams are of nice importance. Extension of the anesthetic into the epidural or subdural areas is theoretically attainable by both dural sleeves or leakage through intervertebral foramen; thus, patients who undergo such procedures should be noticed very rigorously. When the block is performed bilaterally, bilateral phrenic nerve block is a doubtlessly serious hazard. If, nonetheless, infiltration has unfold anterior to the prevertebral fascia, then the cervical sympathetic chain might be concerned, with resultant Horner syndrome, and will unfold also to the recurrent laryngeal nerve, leading to hoarseness (34). Both of those problems in a failed block will indicate that, actually, the anesthetic has been injected at a web site superficial to the deep cervical fascia. Despite important preoperative attempts to enhance their cardiopulmonary situations, these patients incessantly pose vital operative dangers. Since the surgical procedures typically are very prolonged, the chance for administering continuous native anesthetics is enhanced by an epidural catheter (36). Because of the poor well being of many elderly patients, invasive hemodynamic monitoring may be required. Thus, it might present a useful form of analgesia for patients with compromised cardiorespiratory reserve who want main prolonged head and neck reconstructive surgery (38). Regional Anesthesia of the Ear the pinnae of the ear are equipped by both cervical plexus and trigeminal nerves. The cervical plexus branch of the nice auricular nerve (and possibly the lesser occipital) supplies the posterior floor of the ear and the lower third of the anterior surface. The auriculotemporal contribution to the anterior floor of the ear may be anesthetized by infiltration over the posterior facet of the zygoma. A department of the auriculotemporal nerve supplies the inside of the auditory canal over its superior facet, and is injected on the junction between the bony and cartilaginous elements of the anterior wall of the auditory canal, the place it might be reached with a 5- to 6-cm needle. Subcutaneous infiltration at this osseous cartilaginous junction is often accomplished with 2 mL of 1% lidocaine with 1:200,000 epinephrine. The external pinna can be anesthetized using a superficial cervical plexus strategy and by blocking the nice auricular nerve (30). The flooring of the exterior auditory canal and the decrease part of the tympanum are provided by a branch of the vagus nerve. However, like all other forms of remedy and intervention, adverse effects including postinjection an infection, local tissue trauma, and hematoma; allergic reactions may be seen with head and neck blocks (Table 17-12). There are also some particular issues peculiar to regional anesthetics on this space.
Buy cheap forxiga 5 mg line
The authors reported a 70% success rate with one or two needle passes blood glucose unit of measure generic 10 mg forxiga free shipping, and just one failure diabetes type 1 stomach pain buy cheap forxiga 5 mg, in a diabetic affected person (92) diabetes in dogs information purchase forxiga 5mg with amex. The goal response is an evoked muscle contraction beneath the knee; stimulation of the tibial nerve element produces plantar flexion and inversion of the foot, and customary peroneal nerve stimulation produces dorsiflexion and eversion. If no motor response is elicited, the needle may be redirected 1 to 2 cm medially or laterally to the original direction of the needle. It may be useful to palpate or visualize the groove that may be seen or palpated on the posterior side of the thigh. Technique: Sciatic Nerve Block Anterior Approach the anterior approach to the sciatic nerve has the attraction of supine positioning and a single prep of the patient for combined femoral and sciatic nerve blocks. Its reputation had long been limited by its low success fee and relatively painful use of the femur as a deep landmark (94,95). A line that represents the inguinal ligament is trisected, and a perpendicular line from the junction of the middle and medial thirds of this line is extended downward and laterally on the anterior facet of the thigh. The larger trochanter is located by palpation and a line extended from its tuberosity medially across the anterior surface of the thigh, parallel to the inguinal ligament. A 10- to 15-cm needle is inserted via a wheal at this level and directed slightly laterally from a plane perpendicular to the pores and skin. The needle is advanced till bone is contacted, then withdrawn and redirected medially and extra perpendicularly to move 5 cm past the femur, where it must be resting slightly posterior and medial to the femur throughout the neurovascular compartment (containing the sciatic nerve). Technique: Subgluteal Sciatic Nerve Block (Posterior Approach) A posterior subgluteal approach to the sciatic nerve was first described by Ichiyanagi in 1959 (93). Other investigators have described a excessive success fee using this excessive lateral approach with a barely extra caudal entry point (84). When utilizing this strategy, the success price of the blockade of the posterior cutaneous nerve of the thigh was 83%. This may have implications for sufferers undergoing knee surgery or procedures requiring the utilization of a thigh tourniquet. With this strategy, the patient is positioned laterally in a modified Sims position: the leg to be blocked is rolled forward onto the flexed knee because the heel rests on the knee of the dependent (nonoperative) leg. This method is predicated on the bony relationship to the greater trochanter and the ischial tuberosity. The most distinguished elements of the larger trochanter and the ischial tuberosity are identified by palpation, and a line is drawn joining these two factors. The web site of the needle insertion could also be at the intersection of the 2 strains or as far as 6 cm distally along the second line. Technique: Subgluteal Sciatic Nerve Block (Lithotomy Approach) Raj described a supine strategy to the sciatic nerve within the flexed hip (lithotomy) position, initiating the block on the midpoint between the higher trochanter of the femur and the ischial tuberosity (87). The affected person is placed supine, and the extremity to be blocked is flexed at the hip (90�120 degrees). The extremity could additionally be supported by stirrups, mechanical devices, or by an assistant. In this position, the gluteus maximus muscle is flattened and the sciatic nerve relatively more superficial, lying in the readily palpable hole between the semitendinosus and biceps femoris muscular tissues. A line is drawn between the ischial tuberosity and the larger trochanter, and a wheal is raised at its midpoint. A 10to 15-cm insulated needle is inserted perpendicular to the pores and skin and superior till a motor response involving the foot or ankle is elicited. Technique: Sciatic Nerve Block (Lateral Approach) A lateral strategy to the sciatic nerve has additionally been described (84). The earliest report of a lateral strategy was by Ichiyanagi in 1959; it was thought by many to be "extraordinarily difficult" (93). The quadratus femoris is the lowermost of the short rotators of the hip, crossed by the sciatic nerve on its way to the posterior compartment of the thigh. The subgluteal area, within which the sciatic nerve lies as it crosses this muscle, may be recognized in relation to the femur and the ischial tuberosity. The patient lies supine with the whole limb exposed and with the hip held in the pure position. Upon striking the bone of the femoral shaft, the needle is redirected to slide underneath the femur and is advanced to a complete depth of eight to 12 cm to reach the sciatic nerve. The nerve stimulator may elicit responses from both of the motor components of the sciatic. It does carry some sympathetic fibers to the extremity, nevertheless, and may, subsequently, permit pooling of small portions of blood- often insufficient to trigger vital hypotension. On some events, corresponding to limb reimplantations and sympathetically mediated ache situations, this sympathetic block could additionally be advantageous. The effect of compensatory vasoconstriction on the opposite extremity should, nonetheless, be thought-about. Thus, considerate software of this system is required to optimize neurologic end result for sufferers considered to be at excessive risk of perioperative nerve injury from surgery or preexisting neurologic dysfunction. However, theoretical issues regarding muscle trauma and puncture of a big selection of vascular structures, must be thought-about. As these muscular tissues are traced distally Chapter 14: the Lower Extremity: Somatic Blockade 361 A Indications Popliteal fossa block is chiefly used for foot and ankle surgery (100�102). Short saphenous vein stripping may also be carried out beneath mixed popliteal and posterior cutaneous nerve block (103). Potential benefits of popliteal block over ankle block are improved calf tourniquet tolerance and an motionless foot. The elements of the sciatic nerve may be blocked at the level of the popliteal fossa through posterior or lateral approaches. Patient positioning-prone, lateral (operative aspect nondependent), or supine (with leg flexed on the hip and knee)-may determine the optimum strategy for a person affected person (104). Continuous strategies have been described using each posterior (105�107) and lateral (108) approaches. Technique: Popliteal Fossa Block (Posterior Approach) the basic approach to the posterior popliteal fossa block is with the affected person positioned inclined. However, entry may also occur with the patient in the lateral (operative side nondependent), or supine (with leg flexed at the hip and knee) positions. A triangle is constructed, with the base consisting of the skin crease behind the knee, and the 2 sides composed of the semimembranosus (medially) and the biceps (laterally). A bisecting line is drawn from the apex to the bottom of the triangle, and a 5-cm needle is inserted at a website 5 to 10 cm above the skin fold and 0. However, in an try to block the sciatic nerve prior to its division, a 7 to 10 cm distance has been really helpful (109). The needle is advanced at a 45-degree angle toward the apex of the triangle until a nerve stimulator response is elicited; inversion of the foot is the motor response most predictive of full neural block of the foot (110).
References
- Orton DF, LeVeen RF, Saigh JA, et al: Aortic prosthetic graft infections: Radiologic manifestations and implications for management. Radiographics 20:977, 2000.
- Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: executive summary: a report of the ACC/AHA Task Force on Practice Guidelines. Circulation. 2014;130(24):2215-45.
- Krop IE, LoRusso P, Miller KD, et al. A phase II study of trastuzumab emtansine in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer who were previously treated with trastuzumab, lapatinib, an anthracycline, a taxane, and capecitabine. J Clin Oncol 2012;30(26):3234-2341.
- Ascer E, Veith FJ, et at. lntraoperative outfl ow resistance as a predictor of late patency of femoropopliteal and infrapopliteat arterial bypasses. J Vasc Surg 1987; 5:820.
- De Caterina R, Husted S, Wallentin L, et al. Anticoagulants in heart disease: current status and perspectives. Eur Heart J. 2007;28(7):880-913.
- Seldinger SI: Catheter replacement of the needle in percutaneous arteriography: a new technique. Acta Radiol 39:368-376, 1953.
- Stone GW, et al. Routine upstream initiation vs deferred selective use of glycoprotein IIb/IIIa inhibitors in acute coronary syndromes. The ACUITY timing trial. JAMA 2009;297:591-602.