

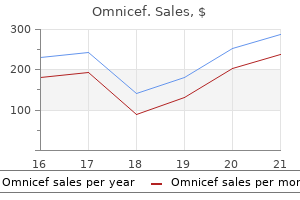
Omnicef
Kathleen Borge, RN, MS
- Faculty Chair
- Samaritan Hospital School of Nursing
- Troy, New York
Omnicef dosages: 300 mg
Omnicef packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills

Order omnicef 300mg with visa
Careful knowledgeable consent included dialogue of emergency airway administration infection 8 weeks after birth trusted 300 mg omnicef, including tracheostomy antibiotics on factory farms purchase omnicef 300mg line, postoperative hemorrhage requiring operative or angiographic control natural antibiotics for sinus infection 300mg omnicef amex, dental harm, tongue numbness or paralysis, style disturbance, and wish for delayed extubation. Lingual tonsillectomy for chronic lingual tonsillitis or hypertrophy or biopsy of suspected lymphoma arising in Waldeyer ring 2. Management of obstructing lingual thyroid or different benign neoplasm of the base of the tongue four. Staging the patient with an occult major of the pinnacle and neck-excisional biopsy of the lingual tonsils and base of the tongue 5. Definitive resection of oropharyngeal (base of the tongue, tonsil, soft palate uvula, posterior pharyngeal wall) squamous cell carcinoma 6. Postprocedure airway administration (extubation, overnight intubation, or tracheostomy) must be discussed with the anesthesia staff prior to the conclusion of the operation. Information gleaned from the preoperative endoscopy and ease of initial intubation should all be thought-about in formulating the plan for postprocedure airway management. Orotracheal intubation using laser-approved endotracheal tubes � T1 or T2 lateral cancer undergoing � Unilateral neck dissection 3. Trismus-Reduced mandible-maxilla excursion with incapability to place acceptable retractors 2. Tumor-Bulky, friable, and/or hemorrhagic tumor obscuring visualization or a tumor with a depth of infiltration into the tongue base that precluded acquiring a satisfactory deep oncologic margin four Tori-Large obstruction maxillary or mandibular tori 5. Tummy-Morbid weight problems is regularly associated with a slender oropharyngeal passage and poor visualization of the most cancers. Tonsils (lingual)-Lingual tonsillar hypertrophy obscuring the view of the tumor and making differentiation from tumor challenging 8. Tilt-Limitations in neck extension from fibrosis from prior radiotherapy, degenerative illness of the cervical spine, or morbid weight problems with unfavorable body habitus 10. Therapy-Prior surgical or nonsurgical remedy can restrict exposure and make differentiation of regular from irregular tissue troublesome. A shoulder roll may not all the time be wanted to facilitate exposure of the oropharynx and the base of the tongue. Patients requiring both a pedicle or free flap reconstruction have their antibiotic protection extended to 5 days postoperatively. Carbon dioxide laser with capability for micromanipulator and fiber supply systems as wanted 2. Identification of the circumvallate papillae defining the junction of the base of the tongue and the oral tongue 2. Hypoglossal nerve programs lateral to the carotid artery and may be encountered within the anterior facet of tongue base Prerequisite Skills Carcinomas of the bottom of the tongue characterize one of the best challenges for the transoral laser microsurgeon. Careful office evaluation of the bottom of the tongue and talent to perform staging endoscopy if needed 2. Ability to convert to open resection of the tongue base by transcervical (suprahyoid or lateral) pharyngotomy 7. Lingual or hypoglossal neuropraxia as a result of pressure from the retractor with resulting anesthesia of the tongue, paralysis, and disturbance of style 4. If the cancer is centrally positioned, this anterior incision is carried across the complete base of the tongue; for more laterally located cancers the incision is terminated at the midline and extends posteriorly. Deep resection margins are established by altering the trajectory of the laser into the base of the tongue. The surgeon should reposition or regularly adjust both the microscope and the retractor system to maintain acceptable visualization and control depth of dissection. Segmental tumor resection may be necessary-that is, bigger cancers are can split into a number of segments with perpendicular laser cuts to facilitate resection. Control posterior margins in the vallecula with the epiglottis retracted inferiorly. Frozen sections of the base of the laryngeal floor of the epiglottis could be obtained at this level. In our own expertise a median of 6 to 7 frozen sections are required for the standard resection of the bottom of the tongue. Clip any pulsatile branches of lingual artery; use thrombin-gelfoam hemostatic material or topical fibrin-based spray. Angled inflexible Hopkins telescopes may be positioned into the mouth both throughout and on the conclusion of the process to examine the defect for bleeding and websites of residual cancer 12. Opportunity to convert to open procedure (lateral or transhyoid pharyngotomy) to complete most cancers resection if necessary b. Pharyngeal perforations or intention pharyngotomy is closed and oversewn and bolstered with native tissue such because the strap muscular tissues or the platysma. Carefully placed suction drains are then used to facilitate coaptation of the neck flap to the neck wound. Assuming most cancers of the tongue base may be excised with out repositioning microscope or changing retractors four. Place dental protectors-Dental harm could be prevented by rigorously inserting any one of numerous commercially obtainable plastic tooth protectors. Custom thermoplastic teeth guards could be fabricated from sheaths of Aquaplast external nasal splint. An appropriately sized retractor is placed just anterior to the foramen cecum, the microscope is positioned, and the initial curvilinear incision is made on the level of the circumvallate papillae. A temporary retention suture positioned in the anterior tongue is useful in establishing and sustaining optimum tongue position. Continue antibiotics for three days if pharyngotomy was closed primarily or with local flap and 5 days if reconstruction was more in depth (pedicle flap or microvascular free tissue transfer). If resection was in depth, speech and swallowing analysis may be wanted previous to resuming oral alimentation. Retractor related because of extreme extension of retractor blades and prolonged strain on the tongue a. Edema and hematoma of the tongue, laceration of the dorsum and lateral tongue, and delayed airway obstruction b. Compression of the lingual nerve between the retractor blade and the inferior border of the mandible, resulting in permanent or short-term disturbance of style and anesthesia of the tongue c. Compression of the hypoglossal nerve between the retractor blade and the hyoid bone, leading to paralysis of the tongue d. Careful consideration to hemostasis by even handed use of the suction cautery, transoral clip hemostasis of recognized bleeding vessels, and elective transcervical ligation of atrisk branches of the lingual, facial, and ascending pharyngeal arteries have been advocated. Infectious complications-Micro- or intentional pharyngotomy within the neck may end up in salivary contamination of the neck with subsequent infection, abscess, or pharyngocutaneous fistula. Primary nonsurgical remedy with definitive concurrent chemoradiation protocols 2.
Discount omnicef 300mg without a prescription
Anatomy of the posterior septal artery with surgical implications on the vascularized pedicled na soseptal flap antimicrobial test laboratories generic omnicef 300mg with amex. Complications related to the pedicled nasoseptal flap for skull base reconstruction antibiotics for sinus infections best ones purchase 300mg omnicef with mastercard. Cerebrospinal fluid diver sion in endoscopic cranium base reconstruction: an evidencebased strategy to using lumbar drains antibiotic 127 300 mg omnicef mastercard. Endoscopic cranium base recon struction of huge dural defects: a scientific evaluation of published proof. The endoscopic skull base surgeon needs to be in a position to select the best reconstruction based on the defect and the needs of the patient. Familiarity with both endoscopic and open techniques is important, especially when the primary recon struction fails. Endoscopic cranium base re development: a evaluate and scientific case collection of 152 vascularized flaps used for surgical skull base defects within the setting of intraop erative cerebrospinal fluid leak. Postoperative management after cranium base reconstruction includes all the next, besides a. An ipsilateral nasoseptal flap will not be attainable if tumor includes the following area(s): a. The procedures performed within the clinic recapitulate the identical surgical methods used in the operating room. The methodology, preparation, and calming bedside manner while performing procedures in the clinic can lead to a trusting patient-physician relationship. Sedation-based or common anesthesia will doubtless be required for kids, anxious or uncooperative adults, the patient with a slender ear canal, and for advanced or time-consuming procedures. A thorough discussion with the affected person regarding expectations regarding the duration of the process, levels of pain, noise concerned, and the potential for vertigo will have a constructive impression on overall satisfaction. The affected person must be knowledgeable that this method will trigger a temporary burning sensation lasting seconds. However, options of 4% to 10% lidocaine (amide) in saline or 8% to 10% tetracaine (ester) in isopropyl alcohol are the most generally described preparations. With the patient positioned supine with the head turned away, the medial half of the ear canal is filled with the predetermined anesthetic agent. The tympanic membrane should be treated for approximately 15 minutes for lidocaine and 60 minutes for tetracaine. Use of a cotton pledget or an otowick positioned within the ear will permit the patient to ambulate whereas allowing the allotted time to lapse. Before commencing with the surgical procedure, the solution ought to be eliminated completely from the canal and the location ought to be tested to guarantee correct anesthesia. As the surgical website expands in size, the options for anesthesia advance from topical brokers and local anesthesia to regional blocks. The ear should be meticulously cleaned to ensure that a topical agent to be efficient. Anesthetic Options for the External Ear and Canal Procedures involving the external ear typically can be carried out within the outpatient setting. Depending on the positioning and extent of the process, topical, native, or regional anesthetics might be thought-about. It is used sparingly in a linear focal region for myringotomy and small focal regions for intratympanic injections. A phenol applicator Topical Anesthesia the good factor about providing an anesthetic with out the need of a needle stick is favorable in youngsters and in sure adults. The site is then examined with a pinprick to be able to be positive that an appropriate degree of anesthesia has been achieved. Auditory branch of the vagus nerve Auriculotemporal nerve Helix Anthihelix Local Injection of Lidocaine With Epinephrine the hemostatic benefits of added epinephrine in injected native anesthetic brokers are well acknowledged. Several studies have demonstrated the secure use of injectable lidocaine with epinephrine in the external ear. Diluting the solution with a 1:10 ratio of bicarbonate to lidocaine will scale back burning on the injection site. A smaller syringe (1 to three mL) will facilitate ease of injection, and a 25-gauge needle or smaller is beneficial. The ache associated with injection will be minimized by injecting slowly, by way of use of distracting measures, and by minimizing the total variety of skin punctures. The most dose of 1% lidocaine with epinephrine is 7 mg/kg as much as 500 mg or 50 mL. The desired effect is generally noted in 2 minutes and may final for 4 to 6 hours. The great auricular nerve and the lesser occipital nerves are branches of the third cervical nerve and cervical plexus. The nice auricular nerve provides sensory innervation to the skin overlying the mastoid process and the inferior pinna. The auriculotemporal nerve, which is a department of the mandibular department of the trigeminal nerve, innervates the superior portion of the pinna. External Ear Block Providing anesthesia to the whole pinna may be useful for remedy of enormous auricular hematomas, laceration repairs, or excisions. A 10-mL syringe is full of 1% lidocaine with epinephrine, and a 25-gauge needle is attached. Without removing the needle completely from the injection site, the direction of the needle is altered to treat the posterior facet of the pinna. In a slim canal or if the canal is occluded by cerumen, the interface between the cerumen and canal wall must be identified. The consistency of the cerumen will dictate the choice of suction, picks, alligator forceps, or curettes. For moist or soft cerumen, aspiration of cerumen is generally probably the most efficient technique of elimination. A 7F suction device ought to be limited to the onset of the procedure if the canal is totally obstructed and ought to be rapidly changed with a 5F system in order to minimize noise publicity. To do this, the lateral canal is full of Colace resolution (docusate sodium liquid, a hundred mg/10 mL) and will stay for 15 minutes previous to continuing with elimination. The degree of issue noted with mastoid cavity care is tremendously depending on the postoperative anatomy of the meatus and mastoid. Some moisture medial to the particles could also be revealed, which can be dusted with Boric acid powder in order to forestall an infection. Excessive moisture may be cleared with suctioning; nevertheless, this generally results in complaints of dizziness. Swabbing the mastoid cavity with cotton held by an alligator forceps or metallic applicator could limit the necessity for suction. A smaller syringe, 1 to three mL, is used to have the ability to present higher dexterity and visibility with a 27-gauge needle. The needle is inserted at the bony cartilaginous junction with the needle advanced a few millimeters alongside the bone. An aural speculum is held with slight strain utilized to the canal wall lateral to the injection website to find a way to encourage medial diffusion of the anesthesia.
Buy discount omnicef 300mg online
If doubtful viruswin32virutce generic omnicef 300 mg fast delivery, the affected person has to be consented for possible total laryngectomy primarily based on intraoperative surgical and frozen section findings infection rate calculation omnicef 300mg with amex. Patients with superior cancer of the tongue usually have poor dentition and should have preoperative dental radiographs done and both be referred to a dentist or have carious enamel eliminated at the time of surgery to prevent subsequent osteoradionecrosis antibiotics for uti delay period purchase omnicef 300 mg line. Finally, the reconstructive group must plan how best to reconstruct the tongue defect and presumably the mandible. Past surgery, trauma, or claudication which will have an effect on the selection of reconstructive flap 3. Second major tongue cancer involving vallecula and epiglottis and requiring total glossectomy with laryngectomy. Pain, salivary pooling, bleeding, and trismus might hamper assessment; due to this fact contemplate administering morphine previous to examination to improve examination. Thickness/height: Thin mandible may preclude marginal mandibulectomy and require segmental mandibulectomy and free fibula flap b. Free fibula (Leg vein harvest and peripheral vascular illness could preclude its use. Not required for cervical metastases as elective neck dissection is at all times done. If concerned about invasion of extrinsic muscular tissues of tongue and suprahyoid straps muscular tissues c. Height of mandible 1) To plan marginal mandibulectomy 2) To determine whether or not segmental mandibulectomy is required d. Perineural invasion of the inferior alveolar nerve might cause widening of the inferior alveolar canal. Prerequisite Skills � Neck dissection: selective ranges 1 to 4; modified; and radical � Total laryngectomy � Mandibulectomy: marginal or segmental � Reconstruction of tongue defect � Pedicled flap: pectoralis major or latissimus dorsi � Free microvascular switch flap: anterolateral thigh, rectus abdominis � Reconstruction of mandible � Plating � Free fibula flap � Tracheostomy Instruments and Equipment to Have Available � Two units of monopolar and bipolar electrocautery for the two surgical groups � Resection and neck dissections � Standard head and neck cancer surgery set � Oscillating saw for marginal mandibulectomy or osteotomies � Mandibular plating set (if required) � Powered drill � Tracheostomy tubes and anesthetic tubing for tracheostomy � Reconstructive surgical procedure (microvascular) � Microvascular instrument set � Microvascular sutures � Ligaclips Surgical Technique � Intraoperative evaluation after patient has been intubated � Panendoscopy to exclude synchronous cancers in upper aerodigestive tract � Reassess extent of primary most cancers, especially posterior and lateral limits. Mylohyoid line and attachments of geniohyoid and genioglossus to inferior and superior genial tubercles and insertion of digastric muscle. Total Glossectomy 205 � Surgical strategy � Good access is crucial to attain enough resection margins, to control bleeding, and for reconstruction. Others favor a midline lip-split incision with median or paramedian mandibulotomy. Incise periosteum along inferior margin of mandible from angle to angle (yellow line), and transect anterior stomach of digastric muscle (green line). Mylohyoid line and attachments of geniohyoid and genioglossus to inferior and superior mental spines; broken line signifies marginal mandibulectomy. Long-term result of pectoralis major flap used to create a convex floor of mouth without sump brought on by retaining the decrease tooth. Common Errors in Technique � Omitting a marginal mandibulectomy and preserving the decrease teeth: the aesthetic benefit of preserving the decrease teeth needs to be weighed towards the reality that the teeth have limited practical value within the absence of a functioning tongue and that the lateral floor of the mouth will function a sump for saliva and meals. In particular, full surveillance for each locoregional and potential distant metastatic illness should be fastidiously attended to preoperatively. After the decision is made to proceed with total glossectomy, the surgeon must have thought-about fastidiously whether laryngeal preservation with the glossectomy is either attainable or fascinating. In my opinion, if significant amounts of the supraglottic larynx require resection or the patient has poor pulmonary reserve that may make tolerance of aspiration poor, complete laryngectomy ought to be performed in conjunction with the glossectomy. The decision to perform a laryngectomy (or not) may also influence the choice regarding the sort of flap reconstruction. Bulk of flap becomes of much less concern within the patient who has a laryngectomy performed in conjunction with the entire glossectomy. If the larynx is preserved, free tissue switch is the popular reconstructive method, whereas pectoralis main myocutaneous flaps symbolize a viable strategy in appropriately selected sufferers. The pectoralis flap is less fascinating in feminine sufferers because of donor web site look, as well as a potentially less reliable skin flap than in males. Because of the long donor pedicle size and high reliability of the flap, coupled with doubtlessly much less donor website morbidity (hernias and closure points in overweight patients), the anterior lateral thigh flap is shortly eclipsing the rectus abdominus and latissimus dorsi flap in our follow. Total glossectomy with preservation of the larynx: oncological and practical results. Patients with superior cancers of the tongue typically have extreme ache and impaired speech, have misplaced a nice deal of weight, and may be cachectic. Blair Cancer of the ground of the mouth accounts for approximately one-third of all cancers of the oral cavity, with squamous cell carcinoma accounting for greater than 95% of circumstances. Despite these similarities, cancers of the floor of the mouth distinguish themselves from different cancers of the head and neck in a quantity of key ways. Perhaps most notable is its propensity for early occult metastasis to the cervical lymph nodes. Although constructive nodal standing is anticipated and even anticipated with advanced-stage cancers (T3/ T4), occult nodal metastasis is a comparatively common discovering, even with early-stage cancer of the floor of the mouth (T1/ T2). Retrospective reviews have demonstrated that as many as 30% of patients with a cancer of the ground of the mouth have evidence of occult nodal metastasis following elective neck dissection. This unique finding makes the remedy of the clinically unfavorable neck a pivotal decision. Advanced-stage cancers of the floor of the mouth pose further challenges, as the intimate anatomic relationship between the floor of mouth and adjoining structures-namely the tongue and mandible-increases the chance of locoregional invasion. As the extent of the cancer increases, so does the associated morbidity of surgical intervention, including compromise of speech, mastication, and oral competence. Together, these distinct oncologic options mix to make cancer of the floor of the mouth one of the more aggressive and doubtlessly lethal neoplasms of the oral cavity. Patient selection and cautious preoperative planning are essential for optimizing oncologic and practical outcomes. Reconstructive efforts ought to aim to provide affordable cosmesis whereas restoring competent physiologic operate to both speech and swallowing. Airway planning, each at the time of surgery and in the course of the postoperative restoration, is critical for limiting morbidity and mortality. The function of the elective neck dissection remains controversial however seems to provide a survival profit. Thus assessment of surgical candidacy sometimes requires a multidisciplinary method, which incorporates evaluations by inside medical specialists, medical and radiation oncologists, speech and swallow therapists, nutritionists, and anesthesiologists. For these deemed match enough to bear surgical resection, the surgeon should subsequent assess the resectability of the cancer. Particular consideration is paid to the presence of native invasion into surrounding constructions of the oral cavity. An accurate evaluation of the connection of the most cancers to the lingual floor of the mandible helps to outline surgical planning and approach. In the immediate preoperative setting, clear and concise communication between surgeon and anesthesiologist is paramount for protected airway management. A retrospective evaluate of 320 sufferers with cancer of the ground of the mouth by Shaha et al. Approaching patient choice as a perfunctory preoperative train is a grave disservice to the patient. However, a diligent history and physical examination, along with a multidisciplinary approach towards surgical optimization, can position the patient for a successful surgical end result.
Generic omnicef 300mg otc
The key to performing secure and efficient ethmoidectomy is understanding the ethmoid cavity anatomy and figuring out critical landmarks in a stepwise trend antibiotic withdrawal symptoms 300mg omnicef for sale. Although the Keros classification is usually described and is necessary for understanding the location of the lateral lamella of the cribriform plate virus 09 purchase omnicef 300 mg overnight delivery, essentially the most helpful relationship in a sensible sense is the relative peak of the maxillary sinus to the height of the ethmoid cavity antibiotic while breastfeeding generic omnicef 300 mg with visa. Once eliminated, the lamina papyracea or medial orbital wall is the primary landmark that should be identified and additional dissected and preserved. Once the vertical basal lamella has been traversed, the third necessary landmark is the superior turbinate. Once the superior turbinate is recognized, the fourth landmark is the cranium base in the posterior ethmoid sinus. The "nook" is a helpful time period to describe the junction of the face of the sphenoid, the skull base, and the orbit. If this level is reached, then the surgeon can be assured that a whole ethmoidectomy may be carried out in a protected method. Key devices essential to carry out a profitable ethmoidectomy embody through-cutting straight and 45-degree upturned mucosal-sparing forceps. The senior creator prefers fine flat jaws compared to the pointed Blakesley shape when eradicating partitions from the skull base. The smaller caliber through-cutting instruments, which are 1 mm in size, may be simpler to maneuver in a narrow ethmoid cavity, in contrast with the standard measurement. A double-ended "J" curette with curved oval suggestions could be useful to take away anterior ethmoid partitions and the ethmoid bulla. Kerrison rongeurs or a sphenoid punch could be useful in removing partitions alongside the lamina papyracea, which are sometimes oriented in the coronal plan. Endoscopic sinus surgeons should be educated of medical remedy that precedes the choice to transfer forward with surgical procedure. The endoscopic sinus surgeon must even have an excellent working information of the sinonasal anatomy and be expert in the utilization of not only 0-degree Hopkins telescopes but also angled telescopes to facilitate dissection of the sinuses. Mucosal preservation is crucial in performing a "useful" surgical procedure, for the reason that functioning element of the sinuses is the ciliated lining that allows for mucous clearance and innate immune regulation. Therefore the ability to precisely use through-cutting instruments is essential in eradicating ethmoid partitions without stripping the lining. Meticulous method by eradicating partitions, avoiding stripping, and making distinct cuts through mucosa-bonemucosa limits bleeding and scarring. Vascular injury to anterior/posterior ethmoid arteries, leading to orbital hematoma four. The mucosa should be anesthetized and decongested with pledgets soaked in a 50/50 mixture of zero. Alternatively, some surgeons choose pledgets soaked in 1:1,000 topical epinephrine. These pledgets should be left in place for at least 10 minutes to maximize topical decongestion. It is important to maneuver the curette in solely the anterior plane to forestall entry into the cranium base (superior) or orbit (lateral). Alternatively a sickle knife can be used to enter the bulla with the purpose dealing with inferiorly, and through-cutting forceps are used to dissect the bulla from the lamina papyracea. Remove residual partitions along the lamina papyracea with a sphenoid punch or Kerrison rongeurs. As one dissects from anterior to posterior, care should always be made to enter cells inferiorly and medially, thus avoiding inadvertent damage to the skull base or orbit. Identify the basal lamella in addition to the roof of the maxillary sinus to determine the trajectory for getting into the posterior ethmoid sinus. The straight portion of the J-curette or a sickle knife is used to traverse the basal lamella and dissect out the bony portion of this construction. Using a microd�brider, the remaining soft tissue of the basal lamella is eliminated to additional outline the anterior head of the superior turbinate. Remove the ethmoid partitions with 45-degree upturned through-cutting forceps, taking care to identify the skull base in essentially the most posterior ethmoid sinus. Partitions which are oriented axially or sagittally can be removed with a straight through-cutting forceps. Identify the junction of the cranium base, anterior face of the sphenoid sinus, and the medial orbital wall. Incomplete removing of the ethmoid bulla and residual partitions left along the lamina papyracea. Failure to identify the superior turbinate completely by inadequately removing the medial portion of the basal lamella as described 3. Failure to totally identify the posterior ethmoid sinuses and the cranium base leading to incomplete ethmoidectomy 5. Incomplete elimination of ethmoid partitions secondary to prior steps not being carried out accurately 6. Counsel the patient to avoid nostril blowing and, if sneezing, to maintain the mouth open to prevent elevated strain within the sinus cavities. Start nasal saline irrigations three times daily, preferably the day of or the day after surgical procedure. We choose a "high quantity, low stress" irrigation (total of 240 mL of saline cut up between every nostril). Patients with nasal polyposis at our institution are treated postoperatively with methylprednisolone 32 mg every day for 7 days and then a 3-week taper (32 mg every different day for three doses, 24 mg each different day for 3 doses, sixteen mg every other day for three doses, and off). Removal of ethmoid partitions alongside the skull base with a through-cutting instrument. This most often happens from failure to establish the lamina papyracea at the onset of surgery in addition to with obstructive nasal polyposis and bleeding. Editorial Comment Endoscopic ethmoidectomy, primary and revision, remains a supply of issues and medicolegal points for the otolaryngologist. The effect of the whole intravenous anesthesia compared with inhalational anesthesia on the surgical subject throughout endoscopic sinus surgery. Is it protected to decrease hemodynamic parameters to achieve cold surgical subject during transnasal endoscopic procedures Clinical effects of middle turbinate resection after endoscopic sinus surgery: a systematic evaluation. Surgery is usually only offered after failure of tried acceptable medical management, as mentioned previously. Symptomatic sufferers should undergo directed medical remedy prior to surgical consideration. At a minimal, this normally consists of culture-directed antibiotics given for so lengthy as sufferers are steadily improving (often 3 to four weeks), nasal steroid sprays, a brief course of systemic steroids, and occasionally topical antimicrobials. Patients whose circumstances warrant exception from a preoperative trial of medical remedy embody these with impending orbital issues, these with mucocele, and those with unilateral illness by which a diagnosis is required to evaluate for diseases apart from persistent nonspecific sinus irritation. The anatomic arrangement of the cranium base with respect to the depth of the olfactory sulcus c.
Omnicef 300mg amex
On occasion a staged procedure is necessary by which efforts are made to initially acquire an intact tympanic membrane and potential center ear house by inserting Silastic sheeting in the middle ear antimicrobial boxers order 300 mg omnicef visa. Anticipating the need for this course of action should be shared with the affected person when the operative procedure and postoperative course are defined antimicrobial carpet purchase omnicef 300 mg with amex. As mentioned bacteria kit order omnicef 300 mg online, surgical procedure of the tympanic membrane is commonly done in conjunction with mastoidectomy and ossicular chain reconstruction. The reader is encouraged to review Chapters 132 and 134 for more details about ossicular chain reconstruction and mastoidectomy. The button graft technique for perforations affecting less than 25% of the tympanic membrane: a non-randomised comparability of a new modification to cartilage tympanoplasty with underlay and overlay grafts. Cartilage tympanoplasty: indications, strategies, and outcomes in a 1,000-patient sequence. There is an extended studying curve to mastering interpretation of the tympanic membrane and center ear findings and the operative strategies wanted to efficiently obtain an intact tympanic membrane, aerated center ear area, and minimal conductive hearing loss. With expertise in executing the intraoperative steps and managing the postoperative care, the surgeon comes to anticipate what intervention will be needed to achieve the desired outcomes. The authors have shared their experience with operative restore of the tympanic membrane. They identified factors that are necessary to obtain profitable grafting of the tympanic membrane. The status of the center ear mucosa and practical integrity of the Eustachian tube are important points that must be recognized. In lateral graft strategies, placement of a healthy fascial graft onto however not extending beyond the annulus minimizes the complication of blunting and persistent conductive listening to loss. Rimming of the perforation is a required step during which of the next tympanoplasty strategies Which of the following is a risk issue for postoperative intratympanic cholesteatoma A near-total perforation Bonus images for this chapter could be found within the ebook at ExpertConsult. Does concomitant mastoidectomy improve outcomes for patients undergoing restore of tympanic membrane perforations Inner ear conductive listening to loss additionally happens when a "third window" exists in the otic capsule. Dehiscence of the superior semicircular canal supplies a site for enlargement of inside ear fluid, which prevents the fluid wave from providing full stimulation to the basilar membrane of the cochlea. This might result in conductive hearing loss despite the precise fact that acoustic reflexes will still be current. Conductive hearing loss of center ear origin could additionally be congenital or acquired and results from ossicular chain fixation, erosion, dislocation, or fracture. Mass impact from reactive gentle tissue processes, tumors throughout the middle ear, and cholesteatoma can also dampen the transmission of sound vitality to the oval window. Tympanic membrane grafting, surgery for stapes fixation secondary to otosclerosis, and continual otitis media with cholesteatoma are addressed in other chapters (Chapters 131 and 133). Tympanoplasty the time period tympanoplasty describes procedures that tackle the standing of the middle ear from the tympanic membrane to the vestibule. Zollner and Wullstein have been early pioneers within the concepts of center ear reconstructive surgery. Each sort refers to probably the most lateral intact structure that remains related to the inside ear on which the tympanic membrane is grafted or the ossicular chain reconstructed. Type Va designates a real fenestration procedure into the horizontal canal, whereas sort Vb implies that the footplate is fixed or absent. After the vestibule is sealed with a tissue graft, continuity is restored from the oval window to the incus, malleus, tympanic membrane, or graft. This classification system is supplemented by describing the strategy of reconstruction used for every case. This technique incessantly uses the body of the incus, the head of the malleus, or a cortical bone graft. Careful palpation plus inspection of the tympanic membrane and all ossicles is crucial for figuring out whether myringosclerosis and tympanosclerosis, individually or in combination, have triggered the conductive listening to loss. Reconstruction of the ossicular chain calls for a precise connection between the tympanic membrane, graft, or malleus and the stapes, footplate, or vestibule. In order to have efficient continuity, anticipate the ultimate resting place of the tympanic membrane and rigidity with the center ear prosthesis. Reconstruction is completed with the affected person supine and the ear going through up towards the operating room ceiling. Risk factors: Previous surgical procedure, Eustachian tube dysfunction, trauma, inflammatory/granulomatous illness, congenital malformation, cholesteatoma, middle ear tumors, and ossicular chain fixation ensuing from tympanosclerosis b. Associated factors: Is there any related tinnitus, aural fullness, distortions in hearing, ache, drainage, an infection, vertigo, or instability Other: Are there another associated signs, like autophony or the Tullio phenomenon Medical illness 1) Is there a earlier historical past of perforated tympanic membrane, pressure equalization tubes, otitis externa, otitis media, or cholesteatoma Surgical historical past 1) If the affected person has undergone earlier otologic surgical procedure, decide the extent and kind. Evaluation of both ears 1) the integrity of the tympanic membrane and middle ear space is evaluated. Diffusion weighted imaging strategies can be utilized for prognosis of cholesteatoma in tough instances. Indications Conductive hearing loss might result from trauma, persistent Eustachian tube dysfunction, congenital anomalies, chronic otitis media, cholesteatoma, tumors of the center ear area, or ossicular chain fixation resulting from tympanosclerosis. When the ossicular chain have to be disarticulated for access to different center ear pathology three. Hydroxyapatite partial ossicular alternative prosthesis making direct contact with the tympanic membrane. Tuning fork testing with 256-, 512-, and infrequently a 1024-Hz fork is carried out to decide whether conductive listening to loss is present and to estimate the degree of loss. Primary inflammation of the pores and skin of the external canal or inflammation secondary to illness from the center ear requires medical administration to optimize postoperative therapeutic. Patients with an intact tympanic membrane, no historical past of persistent ear illness, and progressive conductive hearing loss most doubtless have otosclerosis (see Chapter 133). The affected person is in supine place with the pinnacle rotated away from the affected ear. Adjust the peak of the table and microscope so that the surgeon is comfortable in a seated place, with his or her arms in a relaxed place and not absolutely prolonged. Cefazolin is most commonly used because of excellent staphylococcal and streptococcal coverage. The tympanomeatal incision for exploratory tympanotomy ought to be 4 to 5 mm away from the posterosuperior annulus. Binocular microscope Complete mastoid and center ear set Monopolar and bipolar electrocautery Full complement of otologic prostheses in inventory 7. Postoperative canal stenosis Surgical Technique the approaches to and strategies for tympanic membrane grafting are reviewed in Chapter 131.
Order 300 mg omnicef free shipping
The operative expertise of the surgeon may be more critical and demanding on this setting bacteria battery buy omnicef 300mg. Training and expertise on this regard comes from procedures performed within the working room infection smell generic omnicef 300mg with amex, where methods could be mastered in a managed setting antibiotic lawsuit omnicef 300 mg lowest price. Intratympanic therapies have transformed the supply and outcomes of beforehand restricted treatment options. Gentamicin instilled into the center ear has offered an excellent technique of controlling vertigo attacks from Meniere illness, avoiding more sophisticated operative interventions. Since the affected person is absolutely awake, it is very important have the office geared up with anticipated medications, dressings, and instruments wanted to complete these procedures. Intratympanic dexamethasone for sudden sensorineural hearing loss: medical and laboratory evaluation. Oral vs intratympanic corticosteroid remedy for idiopathic sudden sensorineural listening to loss. Intratympanic dexamethasone for sudden sensorineural hearing loss after failure of systemic remedy. The doctor should have a reassuring demeanor to put the affected person comfortable in this doubtlessly difficult setting. Which of the next agents can be used for topical anesthesia for office-based procedures in otology What is the incidence of hearing loss with low-dose intratympanic gentamicin remedy for Meniere disease Patients could also be handled in a big selection of settings together with an emergency room, clinic, or office. It is important to note that completely different age- and gender-specific patterns emerge in describing the particular types of international bodies found inside the external auditory canal. Jewelry was by far the commonest overseas physique seen in the younger population, with beads and earrings being probably the most regularly recognized types. Senior citizens are also uniquely susceptible to the accidental insertion of disk batteries owing to altered cognition, lowered tactile sensation, and the extra frequent use of hearing aids. The most common inorganic object creating this problem, as already stated, is the tip of a cotton-tipped applicator. Institutionalized adults and kids might use these supplies instead of cotton-tipped applicators, medical packing, or earplugs. In this population, if drainage, an infection, or odor has not developed, such materials may be discovered solely on routine physical examination. Along with using instrumentation to clear their ears, adults also place objects within the ear canal for cover, together with units to reduce water exposure due to recurrent otitis externa or perforation of the tympanic membrane. Materials used for listening to safety can turn out to be lodged or break off and stay in the external canal. Examples of such products embody silicone putty used for sound or water protection and Silastic occlusive plugs or foam inserts for sound safety. Again, sufferers turn into conscious about damaged off supplies remaining in the ear canal. Unless a witness observes a baby putting a foreign physique in the canal, its presence is in all probability not found until routine physical examination detects the item or problems arise because of its presence. Localized aural discharge, cellulitis of the concha and exterior meatus, or serosanguineous otorrhea would prompt further analysis. Once water enters the external canal, vegetable materials corresponding to beans and peas can swell and cause obstruction, ache, and maceration. Other materials that have been found within the ear canal include small toys, beads, erasers, crayons, pits from fruit, disk batteries, nuts, and stones. Disk batteries must be removed as soon as potential to avoid the liquefaction necrosis that results when moisture and secretions permit the move of electrons. Similarly, unsuccessful makes an attempt at removing of the battery that result in trauma and bleeding in the ear canal would additionally permit circulate of current and thus lead to further tissue destruction. Insects sometimes find their method into the ear canals of youngsters and adults alike. These are usually flying bugs, but crawling insects may enter the canal, especially when an individual is sleeping. Patients turn into aware of such a scenario due to the noise generated by the insect and the associated pain. Management in this state of affairs turns into more pressing than that referred to as for by inanimate objects. Live insects ought to be drowned with alcohol, mineral oil, or topical anesthetics (Pontocaine, Xylocaine). A giant nasal suction (10-12 French) device could make enough contact with the thing to take away it from the canal. Passing a right-angled hook parallel to the thing after which past it permits optimum placement of devices for extraction. Injection of an area anesthetic adopted by canal dilatation with progressively bigger specula might facilitate removing of the international body. Ease of extraction is immediately proportional to the variety of earlier failed makes an attempt. Surgery 1) If there was previous otologic surgery, decide its extent and sort. Permits planning when it comes to the appropriate instrumentation, lighting, the sort of anesthesia (if needed), and the tactic of extraction 2. Exploration of the ear underneath intravenous sedation or common anesthesia must be considered for sufferers who might have damage to the ossicular chain or internal ear. General anesthesia will most likely be needed for most kids and anxious, uncooperative adults. Patients with acute hearing loss and dizziness should be suspected of damage transmitted to the internal ear. Positioning � Position the patient so that a head rest is seated comfortably, stabilizing the pinnacle. Consider if patient has a history of in depth otologic surgery, disease, or the medial extent of the overseas body is in question three. Preoperative Antibiotic Prophylaxis � Clean contaminated process � Preoperative antibiotics are typically not required. Hearing loss Instruments and Equipment to Have Available � Binocular otologic microscope � Hydrogen peroxide, isopropyl alcohol, mineral oil � Injectable lidocaine with epinephrine, syringe, and 25-gauge needle � Otologic specula Contraindications 1. Foreign Bodies of the External Auditory Canal 849 � Size: three, 4, 5, and 6 mm � Suction and suction suggestions � Size: 3, 5, 7, 10, and 12 French � Forceps � Small alligator and Hartman-style forceps � Right-angled hook � Cerumen curette � Wire cerumen loop � Silver nitrate � Cotton-tipped applicator � Ear wick � Ear irrigation package (rarely used) 126 Key Anatomic Landmarks 1. A large-gauge suction is normally profitable in removing most objects from the external auditory canal. Adult or pediatric patients with otorrhea, listening to loss, and obstruction or occlusion of the ear canal who fail to respond to topical and systemic remedy might have pathology of the center ear and mastoid or foreign our bodies causing their symptoms and findings. A right-angled hook is handed beyond the thing, which is then extracted laterally. Surgical Technique Foreign our bodies could be categorized not only by their chemical composition but additionally by their form and consistency. Understanding the bodily properties of a overseas physique facilitates the choice of methodology for removing.
Discount omnicef 300 mg otc
Suture tightening: the sutures must be tightened sufficient that the affected person receives maximal profit from an airway standpoint antibiotic 5 day buy 300mg omnicef mastercard. However infection 4 weeks after wisdom teeth removal order omnicef 300 mg visa, tightening them an extreme quantity of could result in antimicrobial effect of chlorhexidine gluconate order 300mg omnicef aspiration or suture breakage, which may require additional surgical procedure. Failure to create subplatysmal dissection tract between skin incisions: this will lead to ugly suture strains underneath the skin. Overnight statement: Patient is saved overnight in a monitored mattress with pulse oximetry. Pain medication: Narcotic ache medication should be restricted to keep away from suppression of respiratory drive, however usually patients are discharged with liquid hydrocodone. Postoperative antibiotics: 1 week of amoxicillin-clavulanate or comparable oral antibiotic Complications 1. Aspiration the inner department of the superior laryngeal nerve provides sensation to the supraglottic airway, and injury may result in aspiration. Seroma and Hematoma A seroma must be drained with a large-gauge needle, and a compressive dressing must be placed. If a hematoma is happening quickly, the incision ought to be opened and the patient should be taken back to the operating suite to get hold of hemostasis. Cellulitis or breakdown of pores and skin incision Treat conservatively with broad-spectrum antibiotics and native wound care. Breakage of suspension material If this happens, further surgical administration shall be wanted. A, the loops of the suspension sutures are placed across the hyoid bone utilizing the working suture. B, Girth hitches are created by pulling the tails of the suspension sutures via the loops and tightening. Other surgical interventions to handle hypopharyngeal collapse: There are a variety of different surgical therapies to tackle base of tongue and hypopharyngeal collapse. These include tongue base discount strategies (midline glossectomy, lingual tonsillectomy, radiofrequency ablation of the tongue), genioglossus advancement, maxillomandibular advancement, and hyoepiglottoplasty. A, Suspension suture is handed inferior to superior on one side and superior to inferior on the contralateral side. Is the efficacy higher or worse than hyoid to thyroid suspension when used as a half of a multilevel airway surgical strategy Original description of the procedure was that of using a fascia lata sling suspending the hyoid from the mandible. This was modified to the hyoid to thyroid suspension to reduce the morbidity of the surgical procedure. There is little within the literature directly comparing the 2 variations of the procedure. Some feel that this is because of the anterosuperior vector of pull on the hyoid with hyoid to mandible suspension, which permits for greater hypopharyngeal displacement than that of the anteroinferior vector of hyoid to thyroid suspension. Others nonetheless feel the hyoid to thyroid method to be less invasive and feel that it adequately stabilizes the base of the tongue and epiglottis, stopping collapse during sleep. Some surgeons additionally feel that hyoid to thyroid may be more successful in male patients versus female sufferers, given the difference in anatomy. More research is needed to better understand the mechanism of motion, handiest surgical approach, and choice of probably the most appropriate surgical candidates. Hypopharyngeal surgical procedure in obstructive sleep apnea: an evidence-based medicine evaluation. The efficacy of multilevel surgery of the higher airway in adults with obstructive sleep apnea/ hypopnea syndrome. Outcomes of hyoid myotomy and suspension using a mandibular screw suspension system. Muscle that inserts into the body of the hyoid at its junction with the higher cornu and must be left intact in hyoid suspension to prevent destabilization of the airway a. The Fujita system for classifying the extent of airway obstruction is usually employed as a diagnostic device. Level 2 indicates obstruction at the retropalatal/oropharyngeal and retroglossal/hypopharyngeal levels. The genioglossus muscle is probably considered one of the major pharyngeal dilators and the first muscle allowing tongue protrusion. The muscle is attached to the genial tubercles positioned on the lingual aspect of the anterior mandible. With many of those procedures, a simultaneous infrahyoid myotomy and hyoid suspension had been usually performed (see Chapter 37). General-A general examination of the affected person is important to assess his or her overall well being and development. Nasal airway-It is essential to totally study the nasal cavity for any evidence of obstruction that might be resolved by way of nasal surgical procedure alone or with a mix of nasal surgery and surgical procedure, affecting one other degree of obstruction. The amount and well being of the keratinized tissue positioned buccal to the mandibular incisors are necessary during the postoperative course, as the incision, closure, and any subsequent scarring are situated adjoining to this space, and contractures might lead to unaesthetic gingival recession around the mandibular incisors. Panoramic Radiograph-To visualize the periodontal tissues, dentition, top of the anterior mandible, psychological foramina, inferior alveolar nerve canal, and temporomandibular joints 2. Lateral Cephalometric Radiograph-Evaluate the presence and severity of maxillary, mandibular, and genial hypoplasia, all of which may contribute to various levels of obstruction in the airway throughout sleep. This is a proven expertise that has been used for years and has been shown to have a high degree of accuracy. Postoperatively, the affected person may be scanned again, and volumetric information could be generated about the improve in airway dimension and capacity. Local anesthesia with epinephrine is useful for postoperative pain management (mental blocks) but is mainly for infiltration into the anterior mandibular buccal vestibule and flooring of the mouth to reduce bleeding and facilitate visualization intraoperatively. Supine place with shoulder roll for partial neck extension Perioperative Antibiotic Prophylaxis 1. Patients concerned about transient or permanent V3 paresthesia Key Anatomic Landmarks 1. The mandibular buccal vestibule is situated between the mandibular incisors and the decrease lip. The mentalis originates from the psychological prominence of the mandible and inserts into the delicate tissues of the chin prominence. The most superior fibers are the shortest and cross almost horizontally into the chin, while essentially the most inferior fibers are the longest and pass obliquely or vertically to the pores and skin on the lower facet of the chin. Oxymetazoline nasal spray previous to the induction of nasal endotracheal anesthesia. Consider perioperative course of high-dose steroids to minimize postsurgical edema of the floor of the mouth, tongue, and airway. [newline]The patient should be intubated for airway protection; ideally, the affected person should have nasal intubation. In the Genioglossus Advancement 403 is innervated by the marginal mandibular department of the seventh cranial nerve (facial nerve). The artery and vein that accompany the nerve are insignificant from a surgical standpoint. However, the mental nerve is a terminal department of the mandibular division (V3) of the fifth cranial nerve (trigeminal nerve), and its operate is to innervate the skin and mucosa of the decrease lip, the facial gingiva of the mandibular incisors, and the skin of the chin. The psychological nerve exits the psychological foramen located near the apex of the primary or second mandibular premolar tooth and usually then splits into three smaller branches that fan out into the area of innervation.

Generic omnicef 300 mg otc
Rehydrate a thick sheet (>1 mm) of acellular human dermis (AlloDerm virus warning discount 300mg omnicef visa, LifeCell) horse antibiotics for dogs purchase omnicef 300mg line, and insert it between the septal cartilage and the flaps virus update order 300mg omnicef overnight delivery. Be certain that the interposition graft covers the entire perforation with no less than 1 cm of overlap if attainable. Secure the graft to the nasal cartilage remnant utilizing 4-0 plain intestine on a straight 11-mm needle. Place interrupted "tacking" mattress sutures posteriorly, superiorly, and anteriorly to safe the graft and prevent motion during last closure. The anterior ethmoid artery flap is then sutured into position at the anterior edge of the perforation, adopted by superior and then inferior sutures. The contralateral flaps are then closed in straight-line trend, with interrupted or operating technique. The bipedicled flaps are then sutured transseptally utilizing a quilting 4-0 plain intestine suture. The Silastic sheets should cover all closure sites, incisions, and areas of denuded cartilage and bone. Patients are instructed to use nasal saline or saline gel in both nostrils 3 to 4 instances every day to present nasal moisturization and promote therapeutic. Patients are instructed to apply the ointment to each nostrils twice day by day to present nasal moisturization and stop localized infection. A first-generation cephalosporin is used to cowl for Staphylococcus aureus whereas the splints are in place. Early intraoperative identification, control with cauterization, heat water irrigation, thrombin base merchandise, and nasal packing 2. Early postoperative identification, drainage, and elimination of lifeless space with mattress sutures 3. Avoid nasal septum mucosal harm superior to the center turbinate pneumatization. Patients are handled with postoperative oral antibiotics, such as a first-generation cephalosporin whereas splints are in place. Consider an open rhinoplasty strategy for improved publicity if an endoscopic approach was attempted first. Failure to elevate the intranasal flaps in the submucoperichondrial or submucoperiosteal plane. Not accounting for flap contracture especially in the anteroposterior dimension four. Not suturing the interposition graft to the septal cartilage remnant resulting in graft displacement throughout closure 5. Very few research, all with low energy, immediately compare the outcomes of different closure methods. Despite this, the general consensus is that long-term closure is finest achieved by way of primary closure using bilateral mucoperichondrial flaps and an interposition graft. Patients are instructed to irrigate both nasal cavities with 240 mL of nasal saline twice every day beginning the morning after surgical procedure. They will continue this via the postoperative interval until nasal mucosal healing is completed. Editorial Comment the repair of a septal perforation stays a challenging process regardless of improved visualization techniques and biomaterials to help the reconstruction. The relative paucity of reconstructive tissue throughout the nostril and the constant airflow dynamics are barriers to successful restore. Nasal septal perforation repair: predictive elements and systemic evaluate of the literature. In addition, prior surgical attempts can additional restrict the reconstructive options and should be thought-about before revision surgery. Finally, the advantages of the reconstruction should also be balanced towards the drawbacks of the restore, specifically the potential for worsening nasal airflow. As with any fistula closure, the use of opposing mucosal vascularized flaps, watertight interpositional grafts, and meticulous gentle tissue handling optimize the probabilities of success. Nasal septum perforation repair using differently designed bilateral intranasal flaps with nonopposing suture traces. Nasal septal perforation remedy methods embrace all the following, besides a. Unilateral flap with major closure and contralateral therapeutic by secondary intent b. Bilateral flaps with primary closure and incorporation of an interposition graft c. Surgery of the turbinate could additionally be an isolated stand-alone process or carried out in conjunction with a nasal septoplasty by which compensatory inferior turbinate hypertrophy may be current on the concave facet of a significantly deviated septum. Abnormally giant turbinates could also be related to anatomic variance or because of pathophysiology, corresponding to rhinitis or rhinosinusitis. The targets of turbinate surgery ought to embody not only the development of nasal airflow but in addition the upkeep of regular physiology. Hence surgical procedure must be performed in a way that preserves the flexibility of the turbinate to condition impressed and expired air, help in mucociliary flow, and sense nasal airflow. This is theorized, although not confirmed, to harm the notion of airflow, possibly by disrupting innervation and mucosal floor receptors. This may end result within the subjective paradoxical expertise of nasal obstruction in an objectively broadly patent nasal cavity, in any other case referred to as "empty nostril" syndrome. Middle turbinate surgical procedure may be necessary as part of a process to address nasal airway obstruction within the case of a concha bullosa and can also be necessary as a key complementary element of nasal septoplasty, as a big concha can forestall efforts to correct a septal deviation. In some cases, a large concha bullosa could also be dissected to improved access to the uncinate process and ethmoid bulla during sinus surgical procedure. In addition, a scarcity of response to nasal decongestants can also help to persuade this patient of the baseline patency of his or her nasal airway. Contemporary methods of turbinate discount ought to maintain a practical mucosal floor that situations impressed and expired air and senses airflow. Overresection of the inferior turbinate mucosa may result in important bony exposure with extreme crusting or may place the affected person in danger for empty nose syndrome. The strategy to the affected person with nasal obstruction ought to embody an assessment of the external nasal framework, inferior turbinates, center turbinates, and nasal septum. It is crucial to respect the uncinate process and ethmoid bulla throughout lateral laminectomy of a concha bullosa to find a way to prevent iatrogenic sinus illness. Medial laminectomy has been demonstrated to be as efficient as lateral laminectomy for aeration of the middle turbinate. Fixed obstruction might happen in the setting of extreme septal deviation or hypertrophy of the inferior turbinate, nasal polyps, or tumor.
References
- Deering RE, Bigler SA, Brown M, et al: Microvascularity in benign prostatic hyperplasia, Prostate 26:111-115, 1995.
- Axelrod D, Preston S. Comparison of parenteral adrenocorticotropic hormone with oral indomethacin in the treatment of acute gout. Arthritis Rheum 1988; 31(6):803-5.
- Packer M, Lee WH, Kessler PD, et al. Prevention and reversal of nitrate tolerance in patients with congestive heart failure. N Engl J Med 1987;317:799-804.
- Light L: Children with enuresis: most cases of primary nocturnal enuresis are caused by isolated developmental immaturity, BMJ 316(7133):777n778, 1998.
- Messerli FH. Case-control study, meta-analysis, and bouillabaisse: putting the calcium antagonist scare into context. Ann Intern Med 1995;123:888-889.